
Download

ORIGINAL ARTICLE
Epidemiology and Clinicopathological Profile of Renal Cell Carcinoma: A Review from Tertiary Care Referral Centre
Likhiteswer Pallagani1, Gautam Ram Choudhary1*, Pandey Himanshu1, Vijay K.S. Madduri1, Mahendra Singh1, Prateek Gupta1, Nikita Shrivastava1, Gaurav Baid1, Rao Meenakshi2, Nalwa Aasma2, Puneet Pareek3, Misra Sanjeev4
1Department of Urology, All India Institute of Medical Sciences, Jodhpur, India;
2Department of Pathology, All India Institute of Medical Sciences, Jodhpur, India;
3Department of Surgical Oncology, All India Institute of Medical Sciences, Jodhpur, India;
4Department of Radio-Therapy, All India Institute of Medical Sciences, Jodhpur, India
Abstract
Renal cell carcinoma (RCC) accounts for 3% of all adult cancers and 85% of all kidney tumours. Incidence of RCC is lower in Asian region, particularly in India, probably due to lack of reporting. Most of the data about RCC are from Western countries; and data from India are scarce, especially regarding para-neoplastic syndromes. We sought to determine the epidemiology, clinicopathological profile and management of RCC in a tertiary care centre in Western India.
This was a retrospective study that involved data analysis of records of RCC patients who presented to our institution from April 2016 to February 2020. Laboratory investigations, including tests for paraneoplastic syndrome (PNS), and relevant radiologic investigations were performed and treatment was offered according to the stage, patient factors and available modalities.
A total 142 RCC patients were included in the study. The median age of presentation was 58 years. Most of the patients (67%) were symptomatic, and 33% of the patients were asymptomatic, and the RCC was diagnosed incidentally. A large number of patients (56.3%) had PNS. The most common histopathologic type of RCC was clear cell carcinoma (68.8%), followed by papillary (20%) and chromophobe (8%) carcinoma. 40% of carcinomas with sarcomatoid differentiation were seen in patients under 50 years of age. Two cases of multicystic RCC were both seen in patients less than 50 years of age. 65.5% of the patients presented at Stage 1 and 2. Most surgeries (71.2%) were done in a minimally invasive manner.
A significant number of patients were asymptomatic, in which RCC was detected incidentally. The age of presentation was earlier, yet the patients had a higher tumour stage. More than half of the patients had PNSs. Despite growing trend towards Western data, the significantly higher number of patients with PNSs and early age of presentation suggest inherent differences in tumour biology, possibly related to differences in genetic and environmental factors.
Key words: epidemiology, laparoscopy, minimally invasive surgery, paraneoplastic syndromes, renal cell carcinoma, robotic surgery, Western India
Received: July 26, 2020; Accepted after Revision: November 25, 2020; Published: January 20, 2021
Author for Correspondence: Gautam Ram Choudhary, Department of Urology, All India Institute of Medical Sciences, Jodhpur, India. Email: [email protected]
How to cite: Pallagani L et al. Epidemiology and clinicopathological profile of renal cell carcinoma: A review from tertiary care referral centre. J Kidney Cancer VHL. 2021; 8(1)1–6
Doi: http://dx.doi.org/10.15586/jkcvhl.2021.154
Copyright: Pallagani L et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0
Introduction
Renal cell carcinoma (RCC) accounts for 3% of all adult cancers and 85% of all kidney tumours (1). Incidence of RCC is lower in Asian region, particularly in India, probably owing to lack of reporting (2). The incidence is expected to rise in India due to increasing life expectancy, rising awareness, better diagnostic facilities and growing prevalence of risk factors such as obesity (3). Most of the data about RCC are from Western countries; and data from India are scarce (4). Because the clinical spectrum of a disease may differ across the globe, this study was undertaken with the objectives of studying the demography, presentation and management of RCC at a referral centre located in western part of India, with the ultimate aim to comment on the clinical heterogeneity of the disease, if any, and to fill the knowledge gap among researchers.
Methods
This is a retrospective study of prospectively kept record, which involved data analysis of records of RCC patients who presented to our institution from April 2016 to February 2020. All the patients had either contrast-enhanced computerised tomography (CECT) scans or magnetic resonance imaging, where renal CECT was contraindicated for clinical staging and characterisation of the renal tumour. Laboratory investigations, including tests for paraneoplastic syndrome (PNS), were performed, and treatment was offered according to the stage, patient factors and available modalities. Renal masses diagnosed as benign were excluded from the analysis. The seventh and eighth edition of the American Joint Committee on Cancer tumour, nodes and metastasis (TNM) staging systems were used to classify cancer stage and grade (5); the seventh edition for cases managed before January 2018 and the eighth edition for cases managed after January 2018. The histological subtypes were classified as per the classification of World Health Organization for renal tumours, 2016 (6).
Results
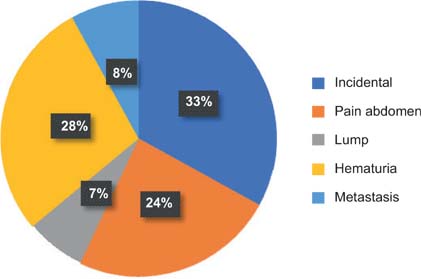
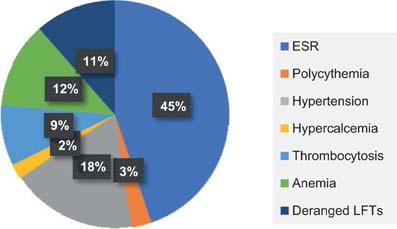
A total of 142 patients vising the institute were diagnosed with RCC, of which 104 patients were male and 38 patients were female. Most patients presented were in the sixth and seventh decades, 43 patients (30.2%) were below 50 years of age. 58 years being the median age at presentation, the youngest patient was 20-year-old and the oldest was 84-year-old (Table 1). Right- and left-sided RCC were equally distributed, and three patients had bilateral tumours. In our study, in many patients, the renal mass was detected incidentally (34%). In symptomatic patients, haematuria (29%) and abdominal pain (24%) were the most common complaints (Figure 1). Nearly 25.6% of the patients had comorbidities, hypertension (HTN) (n = 22) and diabetes mellitus (DM) (n = 17) being the most common (Table 2). PNSs were seen in 56.3% (n = 80) of the patients, with raised erythrocyte sedimentation rate (ESR) (n = 50) being the most common PNS (Figure 2). At presentation, 106 (74.6%) patients were treatment naïve, 31 (21.8%) patients had undergone radical or partial nephrectomy, and 5 (3%) patients had received tyrosine kinase inhibitor (TKI) elsewhere before coming to our centre. Of the 106 treatment naïve patients, 97 underwent surgery as their initial mode of treatment, 9 received TKI upfront and 2 received TKI after cytoreductive nephrectomy. None of the patients who received TKI upfront were deemed fit for any surgical intervention later on. Radical nephrectomy was done in 73 patients, nephron sparing surgery (NSS) in 21 patients and cytoreductive nephrectomy in 3 patients. Most of the radical nephrectomies in our centre were minimally invasive, with conversion to open procedure in three cases. Only cases that were more than 20 cm or involving the adjacent organs or with inferior vena cava (IVC) involvement (level 2) were planned for open surgeries. NSS done in the initial years were open surgeries, but as our institution acquired the da Vinci robotic system, all the NSS in 2019 were robot assisted, of which one was converted to open. The decision to perform NSS was based on the tumour characteristics, patient factors and patient’s choice (Figure 3). Lymph node dissection was done in four cases, of which one case had metastatic deposits. The disease was organ confined (pT1 and pT2) in 93 (65.9%) patients; however, only 26 patients had a tumour size of <4 cm (pT1a). IVC thrombus was seen in 13 patients, most common being level 1 (n = 7), followed by level 2 (n = 4) and level 4 (n = 2). There was no significant difference in clinical stage of the tumour, tumour size, tumour grade, presence of lymph nodes and IVC thrombus in different age groups (Table 3). Of the 106 patients who were treatment naïve, the most common histopathologic type of RCC was clear cell carcinoma, comprising 73 (68.8%) cases, followed by papillary (20%) and chromophobe carcinoma (8%). The other rare tumours were peripheral neuroectodermal tumour (PNET) (n = 2), tubulocystic RCC (n = 1) mucinous tubular and spindle cell carcinoma (n = 1) and solitary fibrous tumour (n = 1) (Table 4). Although clear cell RCC was the most common histologic type in younger age group patients (<50 years), seen in 70% (n = 19) of the patients, the uncommon histologic types were also seen most commonly in this age group. Two patients with sarcomatoid differentiation and two patients with multicystic variant were both <50 years old. Three patients had von Hippel Lindau syndrome, of which two patients had bilateral multiple tumours. One patient with bilateral tumours was managed with cytoreductive nephrectomy and adjuvant TKI and the other patient was managed with upfront TKI and close follow-up. Of total 5 patients with sarcomatoid differentiation, in 2 adjuvant treatment was indicated and chemotherapy (gemcitabine + doxorubicin) was administered, both at 12 months follow-up were recurrence free.
Table 1: Age at presentation.
| S. No. | Age group | No. of patients (n = 142) |
|---|---|---|
| 1 | 0–20 | 1 |
| 2 | 21–30 | 3 |
| 3 | 31–40 | 16 |
| 4 | 41–50 | 23 |
| 5 | 51–60 | 42 |
| 6 | 61–70 | 41 |
| 7 | 71–80 | 13 |
| 8 | 81–90 | 2 |
Table 2: Comorbidities.
| S. No. | Comorbidities | No. of patients (n = 48) |
|---|---|---|
| 1 | Hypertension | 22 |
| 2 | Diabetes mellitus | 17 |
| 3 | von Hippel Lindau syndrome | 2 |
| 4 | Coronary artery disease | 3 |
| 5 | Chronic obstructive pulmonary disease | 2 |
| 6 | Hypothyroidism | 2 |
Table 3: Stage at presentation.
| S. No. | Clinical Stage | No. of patients (n = 142) |
|---|---|---|
| 1 | T1a | 26 |
| 2 | T1b | 31 |
| 3 | T2a | 27 |
| 4 | T2b | 10 |
| 5 | T3 | 19 |
| 6 | T4 | 12 |
| 7 | Metastasis | 17 |
Table 4: Histopathology in patients <50 years of age.
| S. No. | Type of RCC | Number (n = 25) |
|---|---|---|
| 1 | Clear cell carcinoma | 13 |
| 2 | Sarcomatoid variant of clear cell carcinoma | 2 |
| 3 | Multicystic variant of clear cell carcinoma | 2 |
| 4 | Papillary carcinoma | 3 |
| 5 | Chromophobe carcinoma | 2 |
| 6 | Tubulocystic RCC | 1 |
| 7 | PNET of kidney | 1 |
| 8 | Solitary fibrous tumour | 1 |
Figure 1: Presentation.
Figure 2: Paraneoplastic syndrome.
Figure 3: Surgeries.
Discussion
According to available literature, RCC is a disease of elderly population (7). Although data from a developing country like India are limited, as per the SEER database, almost 50% patients with RCC present in the age group between 55 and 75 years and the median age at presentation is 64 years (8). The median age of presentation in this study was 58 years, with one-fourth (26.7%) of the patients less than 50 years of age, and 14% below 40 years of age. This shows a much younger age of presentation in this area. These findings are similar to other Indian studies and Asian studies (4, 9–14). Asian population has a reportedly low incidence of RCC, which may be multifactorial, including genetic and environmental factors or other factors like low reporting (15). The younger age of presentation may also be attributable to environmental factors, dietary factors or genetic susceptibility, which needs to be conclusively addressed by larger epidemiological studies (16). As per existing literature from developed world, the male to female ratio of RCC patients is 2:1 (17). We found an even higher incidence of renal cancers in males, with a male to female ratio of 2.7:1. This finding is similar to that of other Indian studies (2.9) and Asian countries (13, 18). This may be due to the lower incidence of smoking among women or low socioeconomic conditions, leading to difference in treatment seeking behaviour (19).
In our study, most of the patients were symptomatic (67%) with most common presenting symptom being haematuria (28%) followed by pain abdomen (24%), and incidentally diagnosed RCC accounting for only 33%. This is in contrast to findings in Western studies where more than 60% of renal cancers are diagnosed incidentally (20). The incidence of incidental RCC is still higher in our data compared with other Indian studies (4). Similar findings have been noted in another Indian study (21). This could be due to the changing trend towards earlier detection of RCC in India.
It has been established in literature that approximately 20% of patients with RCC develop PNSs (22, 23). These data have predominantly been derived from Western population. In our study, 56.3% patients developed PNS, with raised ESR being the most common (62.5%), followed by hypertension (25%), anaemia (17%), deranged LFTs (16%), thrombocytosis (12%), polycythaemia (4%) and hypercalcaemia (3%). The postulated mechanisms for PNS in RCCs are elevated cytokines (especially IL-6), tumour secreting hepatotoxins and lysozymes (hepatic dysfunction/Stauffer syndrome), renin and IL-6 secretion by tumour cells (hypertension), erythropoietin secretion by tumour cells (polycythaemia), thrombopoietin secretion by tumour cells (thrombocytosis), chronic disease, poor nutritional status and increased iron-binding protein Lactoferrin (anaemia) (21). Immunohistochemistry (IHC) is not routinely applied to the tumour slides for demonstration of tumour cell production of the paraneoplastic agent. Interestingly, hypercalcaemia, which has been noted to be a common PNS in RCC, was found to be the least common in our study (15, 24). This study is the first that highlights the incidence of PNS in the Indian population, and the figure is significantly higher. The reason for the high incidence of PNS could be higher stage of presentation in Indian population, or it could be due to genetic or environmental factors, which need to be further studied.
With respect to histopathology and stage, there are varied data published in the Indian population. The data of histopathology from Western countries show clear cell RCC to be the most common variant, accounting for close to 85% (25, 26). In our study, clear cell RCC accounted for only 68.8% of all tumours. In patients less than 50 years of age, the multicystic variant was more common than in older patients. Moreover, 40% of the patients with sarcomatoid differentiation (2/5) were also <50 years of age. These findings are in variance from those of other Indian studies (4, 10), and from most of the Asian studies (12, 18), which show similar findings as those from the Western population. Only one other Indian study shows similar findings (9). In addition, in our study population, younger patients had varied histological pattern, with higher chances of aggressive carcinoma. Stage at presentation in our patients was also different from those in the West. SEER data suggest that 60–70% of their patients present at Stage 1 (8), but in our study only 40% cases presented at Stage 1 and 65.5% of patients presented at Stages 1 and 2, this shows an advanced stage at presentation of patients with RCC in India compared with Western counterparts where they present at a much earlier stage. This is also reflected in the lower proportion of partial nephrectomies done in this study. Interestingly though, the proportion of patients presenting with localised carcinoma is much higher in this study that other Indian studies (4, 10). This could be because of increased imaging performed in recent years, with widespread use of cross-sectional imaging.
The number of radical nephrectomies done in this study far outweighs the NSS. This is probably due to the higher stage of presentation in our population. Laparoscopic radical nephrectomies were the standard of care rather than exception in our study. Our experience with the laparoscopic surgery has been positive with low open conversion rate (5%) and low morbidity from surgeries. Although the traditional indications for laparoscopic radical nephrectomy are for localised carcinoma (size up to 10–12 cm) (14), we believe there is further scope for expanding these indications to t2b and t3a tumours. Open surgeries still play a role in difficult nephrectomies, for T3b and T3c tumours, and large RCC >15 cm in maximum dimension where placing ports can be difficult; but the indications for it are shrinking day by day. Management of nonlocalised RCC and syndromic patients was discussed in multidisciplinary team and TKI and chemotherapy were used as neo-adjuvant, adjuvant or only treatment modality, according to disease and patient factors.
The limitations of this study are that it was a retrospective study, with smaller number of patients, a few of the patients were operated elsewhere and came to our institution for further management and/or follow-up, and detailed follow-up was not available.
Conclusion
In our study, a significant number of patients were asymptomatic, in which RCC was detected incidentally. The age of presentation was earlier, yet the patients had a higher tumour stage. More than half of the patients had PNS. Clear cell RCC was the most common histologic type, though less common than that is reported in literature. More number of patients less than 50 years of age had sarcomatoid differentiation, with unusual presentations being more common. In conclusion, the findings suggest a growing trend towards Western data. However, the significantly higher number of patients with PNS suggests inherent differences in tumour biology, possibly related to differences in genetic and environmental factors.
Acknowledgements
We would like to thank Mr Tikam Dadhich who helped in the clerical work.
Conflict of interest
The authors declare no potential conflicts of interest with respect to research, authorship and/or publication of this article.
REFERENCES
1. Ljungberg B, Campbell SC, Cho HY, Jacqmin D, Lee JE, Weikert S, et al. The epidemiology of renal cell carcinoma. Eur Urol. 2011 Oct 1;60(4):615–21. 10.1016/j.eururo.2011.06.049
2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018 Nov;68(6):394–424. 10.3322/caac.21492
3. Khandelwal S, Reddy KS. Eliciting a policy response for the rising epidemic of overweight-obesity in India. Obes Rev. 2013 Nov;14:114–25. 10.1111/obr.12097
4. Joshi A, Anand A, Prabhash K, Noronha V, Shrirangwar S, Bakshi G, et al. Kidney cancer demographics and outcome data from 2013 at a tertiary cancer hospital in India. Indian J Cancer. 2017 Oct 1;54(4):601. 10.4103/ijc.IJC_644_17
5. Amin MB, Edge SB, editors. AJCC cancer staging manual. New York; Springer: 2017.
6. Lopez-Beltran A, Scarpelli M, Montironi R, Kirkali Z. 2004 WHO classification of the renal tumors of the adults. Eur Urol. 2006 May 1;49(5):798–805. 10.1016/j.eururo.2005.11.035
7. Thompson RH, Ordonez MA, Iasonos A, Secin FP, Guillonneau B, Russo P, et al. Renal cell carcinoma in young and old patients—Is there a difference? J Urol. 2008 Oct;180(4):1262–6. 10.1016/j.juro.2008.06.037
8. National Cancer Institute. SEER Stat fact sheets: Kidney and renal pelvis. [Internet]. Available at: https://seer.cancer.gov/statfacts/html/kidrp.html
9. Agnihotri S, Kumar J, Jain M, Kapoor R, Mandhani A. Renal cell carcinoma in India demonstrates early age of onset & a late stage of presentation. Indian J Med Res. 2014 Nov;140(5):624.
10. Ray RP, Mahapatra RS, Khullar S, Pal DK, Kundu AK. Clinical characteristics of renal cell carcinoma: Five years review from a tertiary hospital in Eastern India. Indian J Cancer. 2016 Jan 1;53(1):114. 10.4103/0019-509X.180851
11. Singam P, Ho C, Hong GE, Mohd A, Tamil AM, Cheok LB, et al. Clinical characteristics of renal cancer in Malaysia: A ten-year review. Asian Pac J Cancer Prev. 2010 Jan1;11(2):503–6.
12. Kim H, Cho NH, Kim DS, Kwon YM, Kim EK, Rha SH, et al. Renal cell carcinoma in South Korea: A multicenter study. Hum Pathol. 2004 Dec 1;35(12):1556–63. 10.1053/j.humpath.2004.06.011
13. Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA. Campbell-Walsh urology: Expert consult premium edition: Enhanced online features and print, 4-volume set. Toronto, Canada: Elsevier Health Sciences; 2011.
14. Choudhary GR, Mandal AK, Mete U, Mavuduru R, Bhatacharia A, Lal A, et al. Evaluation of quantitative and qualitative renal outcome following nephron sparing surgery. J Clin Imaging Sci. 2018;8:15. 10.4103/jcis.JCIS_82_17
15. Znaor A, Lortet-Tieulent J, Laversanne M, Jemal A, Bray F. International variations and trends in renal cell carcinoma incidence and mortality. Eur Urol. 2015 Mar 1;67(3):519–30. 10.1016/j.eururo.2014.10.002
16. Lipworth L, Tarone RE, McLaughlin JK. The epidemiology of renal cell carcinoma. J Urol. 2006 Dec;176(6):2353–8. 10.1016/j.juro.2006.07.130
17. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020 Jan;70(1):7–30. 10.3322/caac.21590
18. Pang C, Guan Y, Li H, Chen W, Zhu G. Urologic cancer in China. Japanese J Clin Oncol. 2016 Jun 1;46(6):497–501. 10.1093/jjco/hyw034
19. Goggins WB, Wong G. Cancer among Asian Indians/Pakistanis living in the United States: Low incidence and generally above average survival. Cancer Causes Control. 2009 Jul 1;20(5):635–43. 10.1007/s10552-008-9275-x
20. Silverman SG, Israel GM, Herts BR, Richie JP. Management of the incidental renal mass. Radiology. 2008 Oct;249(1):16–31. 10.1148/radiol.2491070783
21. Sacco E, Pinto F, Sasso F, Racioppi M, Gulino G, Volpe A, et al. Paraneoplastic syndromes in patients with urological malignancies. Urol Int. 2009;83(1):1. 10.1159/000224860
22. Palapattu GS, Kristo B, Rajfer J. Paraneoplastic syndromes in urologic malignancy: The many faces of renal cell carcinoma. Rev Urol. 2002;4(4):163.
23. Men H, Liang C, Yu M. Thrombocytosis as a prognostic factor in patients with renal cell carcinoma: A meta-analysis of literature. J Cancer Res Therap. 2015 Jan 1;11(1):67. 10.4103/0973-1482.150345
24. Patard JJ, Tazi H, Bensalah K, Rodriguez A, Vincendeau S, Rioux-Leclercq N, et al. The changing evolution of renal tumours: A single center experience over a two-decade period. Eur Urol. 2004 Apr 1;45(4):490–4. 10.1016/j.eururo.2003.12.015
25. Verhoest G, Veillard D, Guillé F, De La Taille A, Salomon L, Abbou CC, et al. Relationship between age at diagnosis and clinicopathologic features of renal cell carcinoma. Eur Urol. 2007 May 1;51(5):1298–305. 10.1016/j.eururo.2006.11.056
26. Sanchez-Ortiz RF, Rosser CJ, Madsen LT, Swanson DA, Wood CG. Young age is an independent prognostic factor for survival of sporadic renal cell carcinoma. J Urol. 2004 Jun;171(6 Part 1):2160–5. 10.1097/01.ju.0000125487.96469.2e