
Download
REVIEW ARTICLE
Current Options for Second-Line Systemic Therapy in Metastatic Renal Cell Carcinoma
Iraklis C. Mitsogiannis1, Maria Mitsogianni2, Maria Papathanassiou3, Maria Anagnostou3, Ioannis Tamposis4, Lampros Mitrakas5, Maria Samara3, Vassilios Tzortzis5, Panagiotis J. Vlachostergios6*
1Second Department of Urology, National and Kapodistrian University of Athens, Sismanoglio General Hospital, Athens, Greece;
2Fourth Department of Internal Medicine, “Hygeia” Hospital, Athens, Greece;
3Department of Pathology, University of Thessaly, Faculty of Medicine, University Hospital of Larissa, Larissa, Greece;
4Department of Computer Science and Biomedical Informatics, University of Thessaly, Lamia, Greece;
5Department of Urology, University of Thessaly, Faculty of Medicine, University Hospital of Larissa, Larissa, Greece;
6Division of Hematology and Medical Oncology, Department of Medicine, Weill Cornell Medicine, New York, NY, USA
Abstract
Standard systemic therapy of advanced renal cell carcinoma (RCC) involves targeting angiogenesis, mainly through tyrosine kinase inhibitors (TKI) against the vascular endothelial growth factor receptor (VEGFR) pathway and targeting the immune checkpoints, namely, programmed death-1 (PD-1) or its ligand (PD-L1), and cytotoxic T-lymphocyte-associated protein 4 (CTLA4). With current strategies of combining these two approaches in the front-line setting, less is known about optimal selection of therapy upon development of resistance in the second and later lines of treatment for progressive disease. This review discusses currently available therapeutic options in patients who have progressive RCC after prior treatment with double immune check-point inhibitors (ICIs) or ICI-TKI combinations.
Key words: angiogenesis, immunotherapy, renal cell carcinoma, second line, tyrosine kinase inhibitor
Received: 13 June 2022;; Accepted after revision: 26 August 2022; Published: 29 September 2022
Author for correspondence: Panagiotis J. Vlachostergios, Division of Hematology and Medical Oncology, Department of Medicine, Weill Cornell Medicine, New York, NY, USA. Email: [email protected]
How to cite: Mitsogiannis IC, et al. Current Options for Second-Line Systemic Therapy in Metastatic Renal Cell Carcinoma. J Kidney Cancer VHL. 2022; 9(3): 29–40.
Copyright: Mitsogiannis IC, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0
Introduction
Renal cell carcinoma (RCC) is the second most common malignancy of the urinary system and accounts for 4–5% of yearly estimated new cancer cases in the United States (1, 2). Approximately 80% of cases are histologically classified as clear-cell renal cell carcinoma (ccRCC). Advances in diagnostic imaging have led to earlier diagnosis of renal tumors in the last decades (3); nonetheless, 16% of patients initially present with metastatic disease, while recurrences of early stage disease are not uncommon (2, 4). Chemotherapy has shown disappointing results and currently has no place in the treatment of ccRCC (5). The introduction of novel treatments such as immune check-point inhibitors (ICIs) and targeted agents in the first and subsequent treatment lines has substantially improved prognosis for metastatic RCC. However, the reported 5-year survival rates remain as low as 14% (2).
Combined first-line approaches of immunotherapy ICIs and tyrosine kinase inhibitors (TKIs) targeting tumor angiogenesis through vascular endothelial growth factor (VEGF) receptor signaling include pembrolizumab plus lenvatinib, pembrolizumab plus axitinib, and nivolumab plus cabozantinib; these treatment options have demonstrated survival benefit in all treatment-naïve patient subgroups (6–8), whereas double ICIs with nivolumab plus ipilimumab is a valid first-line option for patients with intermediate- and poor-risk disease (9). Single-agent immunotherapy or TKI can be considered in select cases (10). Despite good initial response rates, acquired resistance occurs almost universally. Optimal post-progression treatment sequencing represents a clinical challenge and is highly individualized, depending, to a great extent, on previous regimens, disease burden, biological tumor behavior, and patient’s medical history and health status.
This review discusses currently available therapeutic options in patients who have progressive RCC after prior treatment with double ICIs or ICI-TKI combinations.
Second-Line Anti-Angiogenic Therapies
Treatment with an anti-VEGFR (Vascular Endothelial Growth Factor Receptor), TKI or mTOR inhibitor should be considered for patients progressing on IO or IO-TKI combination and vice versa, although head-to-head comparisons of different agents are lacking and current data to support this approach are based on small studies (11).
Sunitinib
Sunitinib is a multi-TKI inhibitor and was the first targeted agent to be approved in metastatic ccRCC, initially by demonstrating efficacy in cytokine-refractory disease and soon thereafter in treatment-naïve patients when compared to interferon-alpha (12). In recent years, sunitinib has lost ground as the preferred modality in the first-line setting based on the findings of numerous phase III studies of ICI-TKI and ICI-ICI combinations that outperformed it as a comparator arm (11). There are sparse data on the role of sunitinib as a second-line therapy, mostly after prior TKI or cytokine-based therapy and less frequently after ICIs. The RECORD-3 phase II trial demonstrated activity of the everolimus-sunitinib sequence with a median combined progression-free survival (PFS) of 21.7 months and a median OS of 22.4 months, which however was inferior compared to the reverse sequence (sunitinib-everolimus) (13). Rechallenge with sunitinib as third-line treatment and beyond has also shown efficacy supported by a median PFS of 7.9 months (14). In the ICI-based frontline therapy era, prospective evaluation of sunitinib as a second-line agent in the INMUNOSUN-SOGUG phase II trial has yielded a median PFS of 5.6 months and OS of 23.5 months (15). Importantly, those patients who demonstrated better responses to first-line ICI-based therapies were also the ones who benefited the most from sunitinib (15). A larger, real-world retrospective study of 102 patients confirmed the activity of second-line sunitinib following immunotherapy, showing an objective response rate (ORR) of 22.5%, a median time to treatment discontinuation of 5.4 months, and a median OS of 15.6 months (16).
Pazopanib
Pazopanib is a VEGFR-, PDGFR-, and KIT-receptor inhibitor, which is clinically active in metastatic ccRCC, according to the results of a phase III study that included 46% of cytokine-pretreated patients (17). Pazopanib resulted in a longer median PFS compared to placebo (7.4 vs. 4.2 months; HR 0.54; 95% CI 0.35–0.84; P < 0.001) in this pretreated population. However, no survival benefit was shown possibly because of the high crossover rate. Pazopanib is noninferior to sunitinib, in terms of PFS and OS, according to the results of a phase 3 trial in treatment-naïve patients (18); furthermore, the drug has a more favorable toxicity profile and seems to be better tolerated by the majority of patients (19).
Pazopanib was demonstrated to be efficacious in a phase 2 trial, which included patients pretreated with sunitinib or bevacizumab; median PFS and 24-month OS were 7.5 months (95% CI 5.4–9.4 months) and 43%, respectively, regardless of the previously used agent (20). Another single-arm phase 2 study confirmed the efficacy of pazopanib after TKI-failure in cabozantinib or nivolumab noneligible patients (median PFS 6.7 months (95% CI 3.7–11.2), median OS 20.6 months (95% CI 12.6–27.4)) (21). A meta-analysis of six studies further supported the use of pazopanib in noncytokine pretreated patients, despite the lack of robust prospective/randomized data (22). In the post-frontline immunotherapy era, real-world evidence of second-line pazopanib support its safety and efficacy as shown by a median PFS of 13.5 months and a 12-month OS rate of 89% (23).
Sorafenib
Sorafenib is a multi-VEGFR inhibitor and one of the first pharmacologic agents used as targeted therapy in metastatic ccRCC. A phase III trial (24) comparing sorafenib to placebo in pretreated patients reported significantly longer median PFS (5.5 vs. 2.8 months; HR 0.44; 95% CI 0.35–0.55, P = 0.000001). OS was similar, most likely due to crossover. Indirect comparison indicates superiority of cabozantinib, nivolumab, and everolimus over sorafenib as second-line treatment (25). Sorafenib is nowadays reserved for later treatment lines or when other options are not available.
Axitinib
Axitinib is a potent inhibitor of VEGFR-1, -2, and -3. In the landmark phase 3 AXIS trial (26, 27), axitinib was compared to sorafenib as the second line treatment of metastatic ccRCC. Median PFS was longer with axitinib (8.3 vs. 5.7 months, hazard ratio (HR) 0.66, 95% confidence interval (CI) 0.55–0.78, one-sided P < 0.0001). Superiority of axitinib was particularly evident in cases of prior cytokine treatment (PFS 12.1 vs. 6.5 months; HR 0.46, 95% CI 0.32–0.68), compared to prior sunitinib (PFS 4.8 vs. 3.4 months; HR 0.74, 95% CI 0.57–0.96). Overall survival (OS) did not differ significantly between the two groups (20.1 vs. 19.2 months, HR 0.70, 95% CI 0.80–1.17; one-sided P = 0.374) (27). Patient-reported kidney-specific symptoms and health status, measured by the Functional Assessment of Cancer Therapy (FACT) Kidney Cancer Symptom Index (FKSI) and the European Quality of Life self-report questionnaire (EQ-5D) in the AXIS trial were similar between axitinib and sorafenib, with substantial worsening at the end of treatment mainly due to disease progression (28). Longer duration of first-line treatment (cytokines or sunitinib) was positively associated with survival in a post hoc analysis (29). Common adverse events included diarrhea and hypertension, while toxicity led to treatment discontinuation in 4% of patients. Interestingly, high (>90 mmHg) diastolic blood pressure was associated with prolonged overall survival (27).
Prognostic factors associated with better response to axitinib compared to sorafenib, in the sunitinib-pretreated group of patients, include nonbulky, favorable-, or intermediate-risk disease, as well as the absence of liver and bone metastases (30). The efficacy of axitinib in favorable risk sunitinib-pretreated patients was further confirmed in a single-arm, phase 2 study of 21 patients, which reported responses in 33% of patients and a median PFS of 17 months (95% CI 14–20) (31).
Axitinib after immune-checkpoint inhibition has also been prospectively evaluated in a single-arm phase 2 study (32). A total of 40 patients were included, the majority of which (63%) were treated with nivolumab directly before trial enrollment. ICI combination with nivolumab and ipilimumab was the most recently received regimen in 15% of the patients. An ORR of 45% and a median PFS of 8.8 months (95% CI 5.7–16.6) were noticed (32).
Quality-of-life (QOL) analysis using the Medical Outcomes Study 36-Item Short Form in a real-world clinical practice study of 124 patients showed that all eight QOL scores after the introduction of axitinib were superior to those before its introduction, and there were significant differences in two of the eight scale scores between surveys conducted before and 12 weeks after the introduction of axitinib (33).
Cabozantinib
Cabozantinib affects cancer growth by inhibiting VEGFR-2 and other tyrosine kinases, such as MET and AXL, which are associated with resistance to sunitinib and poor prognosis (34). It has been established as a subsequent treatment option of metastatic ccRCC based on the results of the phase 3 METEOR trial (35). Patients progressing on ≥1 VEGFR-TKI were randomized to either cabozantinib or the mTOR inhibitor everolimus. Cabozantinib demonstrated both PFS (7.4 vs. 3.9 months, HR 0.51, 95% CI 0.41–0.62, P < 0.0001) and OS benefit (21.4 vs. 17.1 months, HR 0.71, 95% CI 0.58–0.85, P = 0.002). In subgroup analysis, benefit was maintained irrespective of prior use of ICI. A phase 2 trial evaluating cabozantinib after progression on the current first-line standard-of-care (predefined cohorts of ICI-ICI and anti-VEFGR/ICI combination), is ongoing (36).
Tivozanib
The VEGFR-inhibitor tivozanib is the most recently approved TKI in the treatment of relapsed RCC. It has been evaluated in the randomized phase III TIVO-3 trial, where it was compared to sorafenib after disease progression on at least two treatment lines (37, 38). Clear-cell histology accounted for more than 95% of the cases in both arms. Tivozanib led to an improvement of PFS (6 vs. 4 months, HR 0.73, 95% CI 0.56–0.94) but not of OS (16 vs. 19 months, HR 0.97, 95% CI 0.75–1.24) (38). Benefit was seen in patients who had previously received checkpoint inhibition and VEGFR TKIs and two different VEGFR TKIs (38).
Lenvatinib
The VEGFR-targeting TKI lenvatinib in combination with the mTOR inhibitor everolimus has demonstrated PFS benefit compared to everolimus alone, according to the results of a phase 2 trial (14.6 vs. 5.5 months, HR 0.40, 95% CI 0.24–0.68) (39). It has been approved after failure of antiangiogenic treatment. The approved dose of lenvatinib is 18 mg. It has been tested whether a starting dose of 14 mg is noninferior in a randomized phase 2 trial, but both PFS and OS were numerically better in the 18 mg arm (40). Real world data indicates effectiveness of the Lenvatinib-everolimus combination after prior TKI with a median PFS of 6.4 (95% CI 4.1–10.8), and after immunotherapy with median PFS of 5.7 months (95% CI 4.1–10.5) and median OS of 14.8 months (95% CI, 10.2–23.9), as well as in heavily pretreated patients after a median of 3 previous treatment lines (41).
All available anti-angiogenic agents studied so far in the second line are summarized in Table 1.
Table 1: Randomized trials of second-line agents after VEGFR TKI monotherapy.
| Axitinib | Cabozantinib | Lenvatinib/Everolimus | Nivolumab | |
|---|---|---|---|---|
| Study | Rini et al. (26) | Choueiri et al. (35) | Motzer et al. (39) | Motzer et al. (42) |
| MSKCC risk: favorable/int/poor | 28/37/33 | 45/42/12 | 24/37/39 | 35/49/16 |
| Comparator | Sorafenib | Everolimus | Everolimus | Everolimus |
| ORR, % | 19 | 17 | 35 | 22 |
| PD, % | 22 | 12 | 4 | 35 |
| PFS, mo | 4.8 | 7.4 | 12.8 | 4.6 |
| OS, mo | 20.1 | 21.4 | 25.5 | 25.0 |
Abbreviations: VEGFR, vascular endothelial growth factor receptor; TKI, tyrosine kinase inhibitors; MSKCC, Memorial Sloan-Kettering Cancer Center; int, intermediate; ORR, objective response rate; PD, progression of disease; PFS, progression-free survival; OS, overall survival; mo, months.
Second-Line Immunotherapy
Nivolumab and Ipilimumab
Nivolumab monotherapy is indicated in patients who have progressed on anti-VEGR treatment, based on the results of the CheckMate 025 randomized phase 3 trial (42, 43). Nivolumab was compared to everolimus, and it demonstrated superiority in terms of ORR (23 vs. 4%), 5-year PFS (5 vs. 1%, HR 0.84, 95% CI 0.72–0.99), and OS (25.8 vs. 19.7 months, HR 0.73, 95% CI 0.62–0.85), although median PFS did not differ. Quality of life was also improved in the nivolumab group (42, 43). There are also data indicating the benefits of nivolumab post-progression in patients experiencing clinical benefit (44). Nivolumab after disease progression led to >30% reduction in tumor burden in 13% of the patients who stayed on treatment (44).
The combination of nivolumab and ipilimumab is a valid option for patients who are in good shape and did not receive it as first-line treatment. Salvage therapy with nivolumab and ipilimumab has demonstrated efficacy after progression on anti PD-1 targeted therapy in a small retrospective analysis of 44 patients. ORR was 20% and median was PFS 4 months (45). In another ambispective multicenter study with 45 mRCC patients rechallenged with nivolumab±ipilimumab, ORR was 16% (n = 7) for second-line ICI (45). Median PFS was 3.5 months, and median OS was 24 months (46). Factors associated with poorer PFS were a high number of metastatic sites, presence of liver metastases, and the use of an intervening treatment between ICI regimens, Eastern Cooperative Oncology Group performance status ≥2, and poor International Metastatic RCC Database Consortium score upon second-line ICI initiation (46). Conversely, a PFS longer than 6 months at first-line ICI was associated with better PFS during second-line ICI (46).
TiNivo-2 is a phase III randomized trial comparing nivolumab plus tivozanib to tivozanib monotherapy in metastatic RCC patients who have progressed following one or two lines of therapy including an ICI, with primary endpoint being PFS (NCT04987203).
Pembrolizumab
Pembrolizumab as later-line treatment after failure of ICI has been evaluated in combination with lenvatinib in a phase 1b/2 trial with a total of 104 patients, the majority of which had received at least two treatment lines. The investigators described an ORR of 56%, and median DOR of 12.5 months (47).
Atezolizumab
The combination of atezolizumab and bevacizumab demonstrated activity in patients progressing after atezolizumab or sunitinib. In this randomized phase 2 trial, 103 patients started second-line atezolizumab plus bevacizumab, of whom 44 had previously received atezolizumab as first-line monotherapy while 59 were previously treated with sunitinib (48). ORR was reported as high as 27%. The median PFS from the start of second line was 9 months. The median event follow-up duration was 19 months among the 25 patients without a PFS event (48). Atezolizumab combined with cabozantinib is currently being tested in the pivotal, global phase III CONTACT-03 trial in patients with inoperable, locally advanced or metastatic RCC who progressed during or following treatment with an ICI (NCT04338269).
All available ICI options studied so far in the second line are summarized in Table 2.
Table 2: Prospective and retrospective trials of second-line agents after ICI/VEGF inhibitor or ICI ± ICI.
| Ipilimumab/Nivolumab | Ipilimumab/Nivolumab | Lenvatinib/Pembrolizumab | Atezolizumab/Bevazicumab | |
|---|---|---|---|---|
| Study | Gul et al. (45) | Vauchier et al. (46) | Lee et al. (47) | Powles et al. (48) |
| IMDC or MDACC risk: favorable/int/poor | 20/64/7 | 23/25/53 | 17/59/24 | 21/76/3 |
| ORR, % | 20 | 16 | 62.5 | 27 |
| PD, % | 62 | 67 | 57 | 32 |
| PFS, mo | 4 | 3.5 | 12.2 | 8.7 |
| OS, mo | NR | 24 | 72% at 16 mo | NR |
Abbreviations: VEGFR, vascular endothelial growth factor receptor; ICI, immune check-point inhibitors; IMDC, International Metastatic RCC Database Consortium; MDACC, MD Anderson Cancer Center; int, intermediate; ORR, objective response rate; PD, progression of disease; PFS, progression-free survival; OS, overall survival; mo, months; NR, not reported.
Comparisons between Therapeutic Options in the Second-Line Setting
Several targeted anti-angiogenic agents used as monotherapy have been proved to be more efficient than sunitinib and have further reduced its clinical use. Cabozantinib led to superior ORR (20 vs. 9%) and PFS (8.6 vs. 5.3 months, HR 0.48, 95% CI 0.31–0.74) in treatment-naïve patients with intermediate- and high-risk disease (49).
With regard to treatment sequencing, sorafenib followed by sunitinib on disease progression appears to be equally efficient to sunitinib followed by sorafenib according to randomized, phase 3 data (50). On the other hand, everolimus followed by sunitinib has failed to demonstrate non-inferiority compared to sunitinib followed by everolimus in a randomized, phase 2 trial (51).
Axitinib does not seem to be superior to nivolumab as second-line option after targeted therapy, although a trend towards improved PFS was reported in a small retrospective study (52). Axitinib re-challenge as fourth- or later-line treatment has demonstrated clinical benefit in a recent case series (53).
According to a meta-analysis including patients progressing on VEGFR inhibition (20), cabozantinib was associated with a lower HR for disease progression and death compared to axitinib, everolimus, nivolumab, sorafenib, and best supportive care. It is, therefore, being currently recommended as a preferred second-line option in the latest NCCN guidelines (54). Retrospective real-world data further confirm PFS superiority of cabozantinib vs. nivolumab for ccRCC (7.8 vs. 5.4 months, P = 0.026) and good-risk disease (12.3 vs. 5.7 months, P = 0.022) (55).
Controversies on Retreatment with Immune Checkpoint Inhibitors
From a biological standpoint, there is evidence of continued activity of anti-PD-1 blockade up to 3 months after initial administration and up to 9 months after at least three treatment cycles (56). Furthermore, because the mechanism of action of ICIs is mainly based on their ability to trigger adaptive immune response by reversing the inhibition and suppression of T cells in the tumor microenvironment, whether further continuation of ICI after reactivation of immune response is established is questionable (57). On the other hand, when compared with nonstop treatment with nivolumab for over 1 year, retreatment at progression in the CheckMate-153 trial resulted in inferior PFS and OS outcomes (58).
Even without interruption, patients treated with ICIs eventually experience progression of their disease due to the development of acquired resistance. Resistance mechanisms may involve insufficient generation of anti-tumor T cells, inadequate function of tumor-specific T cells, or impaired generation of memory T-cells (59, 60).
In the absence of predictive biomarkers, clinical phenotypic characteristics could offer some hints to guide the choice and sequencing of ICIs in ICI-pretreated patients. For example, treatment with the same ICI beyond progression might be an option for a subset of patients who experienced slow progression after initial response. On the other hand, patients with primary resistance to ICI as well as those with visceral disease or rapid deterioration might not benefit from this strategy but should rather be offered a course of TKI with faster onset of activity (61). After eliminating the most aggressive cancer clones, altering the tumor microenvironment, removing immunosuppressive signals, and releasing novel tumor-associated antigens, retreatment with a different ICI might be effective (62, 63). Combining ICIs against different immune targets might be one way to prevent or/and overcome resistance and improve outcomes in these patients.
Hypoxia-Inducible Factor 2α Inhibition
Belzutifan is a potent, selective, oral small-molecule HIF-2α inhibitor with antitumor activity in clear-cell RCC (64). The drug at 120-mg dose was shown to be well tolerated and demonstrated significant activity translating into an ORR of 25% and a DCR of 80% in 55 patients with advanced ccRCC previously treated with at least one prior line of therapy (65, 66). While belzutifan is already FDA-approved for patients with von Hippel-Lindau (VHL) disease who require therapy for associated RCC, based on a phase 2, open-label, single-group trial (67), a phase 3 study comparing the drug with everolimus in advanced RCC after PD-1/PD-L1 therapy and TKI is underway (NCT04195750). There is also encouraging evidence of activity and tolerability of belzutifan in combination with cabozantinib in 53 previously treated patients, including immunotherapy and TKIs (cohort 2) (68). The study reported a confirmed ORR of 22% while the disease control rate (CR + PR + SD) was 92.7% and median PFS was 16.8 months (66).
Local Therapies for Oligoprogressive Disease
Cytoreductive nephrectomy and metastasis-directed therapies involving resection, radiation, or ablation, either upfront or after initiation of systemic therapies, continue to have a role in the management of metastatic RCC (67). Their contribution in improving outcomes of patients with oligoprogressive disease after initial systemic therapy is less clear and requires even more careful patient selection due to lack of predictive biomarkers (68). Retrospective data suggest that patients with a Memorial Sloan-Kettering Cancer Center (MSKCC) good risk score or bone metastases may experience longer post-first oligoprogression OS compared to patients of the intermediate risk group (39 vs 29 months) or visceral metastases (not reached vs 31 months), respectively (69). Retroperitoneal lymph node dissection (RPLND) and metastasectomy may be beneficial when technically feasible in oligometastatic disease and a proportion of those may achieve long-term OS with aggressive resection (70). However, postoperative complications should be carefully weighed upon decision-making, particularly in hepatic resections which portend the highest risk for major ones (Clavien III-IV) in up to one-fourth of the patients (71).
Intraoperative cryotherapy may have a role in osseous metastases in controlling the metastatic tumor bed and offering long-term pain relief; however, more data are needed (72). Percutaneous multisite cryoablation may address various anatomic sites under ultrasound- or CT-guidance and is cost-effective further to having only a 2% rate of complications or local recurrence (73). Microwave ablation is also safe with a 15% rate of complications and durable local control in 93% of cases, although retrospective nature and small study size remains a limitation (74).
The most well-studied, noninvasive local approach is radiotherapy, mostly in the form of stereotactic body radiation (SBR). A large amount of prospective and retrospective studies and meta-analyses support the activity of this approach for treating oligometastatic disease in combination with TKIs or ICIs (75). Local control rates usually exceed 90%, even for intracranial disease, with severe toxicity being uncommon (<10%) (75). Although prospective evaluation of SBR plus nivolumab did not add any systemic benefit with respect to ORR (17%) and median OS (20 months) compared to historical controls of nivolumab alone in the NIVES study, more prospective trials such as the RAPPORT study are further investigating this with molecular correlates to provide insights into the underlying biology of combination SBR and ICI therapy (76, 77). With respect to clinical correlates, a good ECOG PS ≤1 predicts a longer OS benefit in such patients (78). Other retrospective studies suggest a greater benefit from SBR in patients with metachronous metastases and in those with smaller lesion size (<14 mm) (79, 80). Complete SBR (as opposed to incomplete SBR) may lead to improved cancer-specific survival in younger patients (age <55 years), with clear-cell tumors and low metastatic of <3 lesions (81). Another outcome often underscored in various studies is time to next systemic therapy initiation or time to systemic therapy escalation, which can be significantly prolonged with SBR for over a year, as well as with classic external beam radiation (82–88). Alternatively, SBR can significantly extend the duration of ongoing systemic therapy by more than 6 months without compromising the quality of life (89). Stereotactic radiosurgery (SRS) can achieve such good local control that the median OS rates after switching systemic therapy versus continuing the same are similar (24 vs 27 months) (90).
Next-Line Treatment Selection
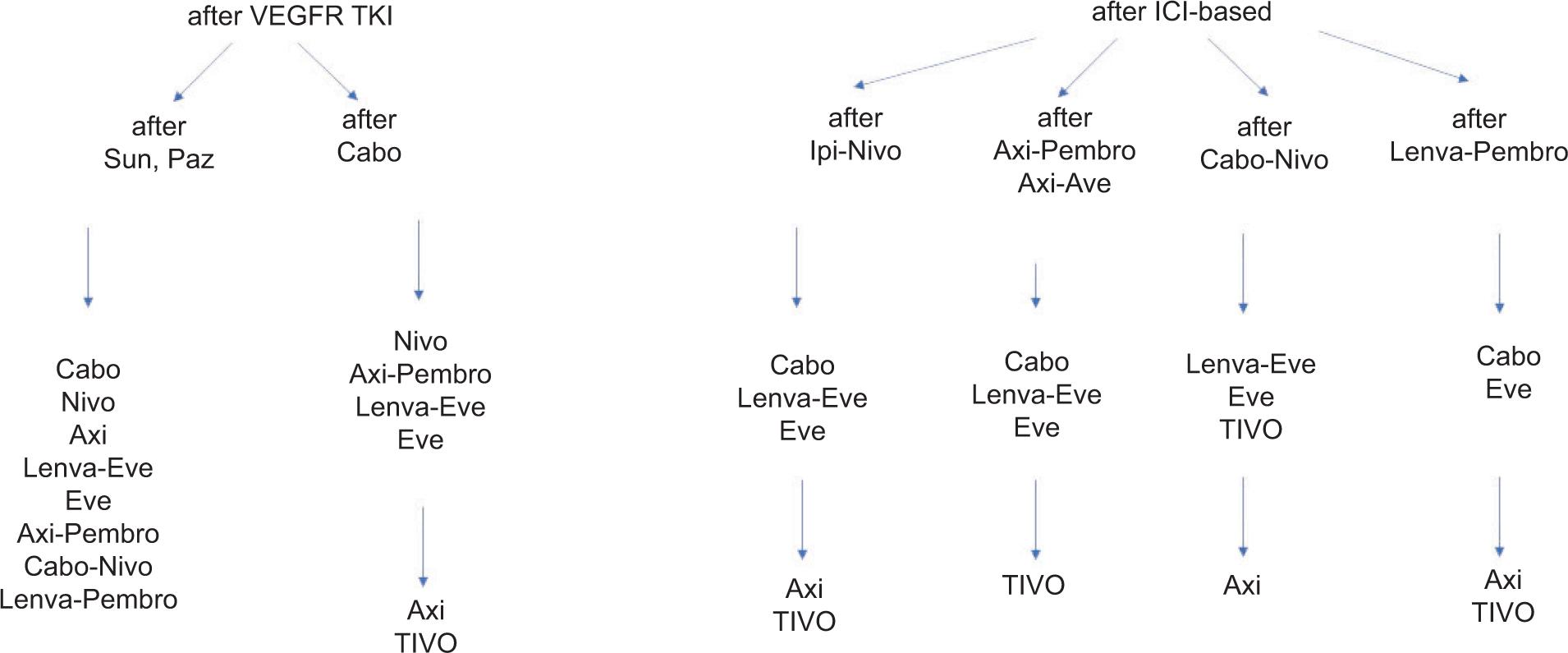
Overall, there are no randomized comparisons between different treatment options for second and subsequent lines of therapy. Based on variable ORR, duration of responses, and PFS in individual studies, some general principles could be proposed. If long-term disease control was previously achieved on first-line single-agent VEGF inhibitor (i.e., pazopanib), patients could either continue VEGF inhibition alone with cabozantinib or axitinib or tivozanib, or in combination with an mTOR inhibitor (lenvatinib and everolimus), or receive ICI monotherapy with nivolumab. Besides, these options are supported by category 1 evidence according to current NCCN treatment guidelines; active second-line regimens include other TKIs (sunitinib, pazopanib), ICI-TKI combinations (axitinib-pembrolizumab, cabozantinib-nivolumab, lenvatinib-pembrolizumab, axitinib-avelumab), or double ICI combination (ipilimumab-nivolumab) (54). After primary or acquired progression on VEGF and ICI combination, non-ICI VEGF inhibition strategies with a different VEFGR-targeted agent should be implemented. According to ESMO guidelines, this strategy is associated with modest response rates and should be considered the standard of care (11). In the absence of strong evidence to support continued ICIs after progression on first-line ICI-based therapy, if disease control was achieved on ipilimumab plus nivolumab prior to progression, consideration could be given to VEGF and ICI combinations for second line, particularly lenvatinib plus pembrolizumab. These same options can be considered for third line and beyond, depending on what the patient has previously received. Proposed treatment algorisms for second- and third-line treatment of ccRCC are illustrated in Figure 1. Until present, therapeutic decisions in this setting are mostly guided by strength of evidence for each drug, its toxicity profile, disease aggressiveness, mechanism of action, and pattern of responses during prior lines of therapy, patient comorbidities, availability of clinical trials, patient and physician preferences, and financial concerns.
Figure 1: Suggested sequences for second- and third-line treatment of clear-cell RCC.
Abbreviations: RCC, renal cell carcinoma; VEGFR, vascular endothelial growth factor receptor; TKI: tyrosine kinase inhibitor; ICI, immune checkpoint inhibitor; Sun: sunitinib; Paz: pazopanib; Cabo, cabozantinib; Nivo, nivolumab; Ipi: ipilimumab; Pembro, pembrolizumab; Axi, axitinib; Tivo, tivozanib; Lenva, Lenvatinib; Eve, everolimus.
Nonclear-Cell RCC
In this minority of clinicopathological RCC subtypes where phase III randomized studies are lacking, preferred frontline therapy consists of a VEGFR TKI, usually either cabozantinib or sunitinib, particularly in papillary tumors, although outcomes are usually inferior compared to ccRCC (11, 54, 91). Another alternative is the combination of lenvatinib and everolimus supported by phase 2 data (92). As a result, subsequent lines of therapy after progression may include either a different TKI or/and an ICI. The combination of cabozantinib and nivolumab demonstrated promising activity in the unclassified/papillary/translocation-associated cohort of a phase II study with a median ORR of 47% and OS of 28 months (93). One third of those patients had received one prior line of therapy with a VEGF or mTOR inhibitor (93). Nivolumab monotherapy in the phase IIIb/IV CheckMate 374 study in previously treated non-ccRCC patients also demonstrated clinically meaningful activity with median ORR of 13% and OS of 16 months (94).
Newer studies, mostly retrospective, have demonstrated improved OS with ICI-based frontline therapy compared to VEGF and mTOR-targeted agents (26 vs 16 vs 12 months, respectively) (95). Safety and efficacy results from the advanced non-ccRCC cohort of the phase IIIb/IV CheckMate 920 study confirmed the activity of first-line treatment with nivolumab and ipilimumab with a median ORR of 19% and OS of 21 months (96). Likewise, pembrolizumab monotherapy in the phase II KEYNOTE-427 study resulted in high response rates of 28.8% for papillary, 9.5% for chromophobe, and 30.8% for unclassified tumors (97). Thus, it is likely that the future landscape of second and subsequent-lines of treatment in non-ccRCC patients may face the same dilemmas and challenges with ccRCC with respect to prior use of ICIs. Furthermore, while systemic therapy rates are increasing contrary to those of cytoreductive nephrectomy alone or in combination with systemic therapy in non-ccRCC, the latter is associated with lower overall mortality in appropriately selected patients (98).
Future Perspective
How the underlying tumor biology may determine responses and resistance after initial therapy remains poorly understood. PD-L1 immunohistochemical expression has shown promise; however, variations in various assays along with use of different cutoffs for positivity are challenging. Several other candidate biomarkers were tested including tumor mutational burden, gene expression signatures, single gene mutations, human endogenous retroviruses, the gastrointestinal microbiome, and peripheral blood laboratory markers (99).
Recent gene expression analysis from the largest randomized trials in the first-line setting, that is, CheckMate 214 support a role for the inflammation status of the tumor microenvironment and PFS with ipilimumab plus nivolumab combination (100). A single-cell transcriptomic analysis of cancer and immune cells from metastatic RCC patients before or after ICI therapy revealed two subpopulations differing in angiogenic signaling and upregulation of immunosuppressive programs associated with PBRM1 mutation (101).
Appropriate selection of next-line therapies in metastatic ccRCC in the current era of ICI-ICI and ICI-VEGFR TKI combinations is challenging and there is a paucity of biomarkers to inform clinical decisions. While there is an urgent need for randomized comparative trials in this setting, given the heterogeneity of treatment responses to immunotherapy, it is unlikely that machine learning will identify a unifying transcriptional signature predictive of ORR (102–104). The BIONIKK study is the first prospective biomarker-driven phase 2 randomized trial in mRCC that will be using a 35-gene signature which reflects intrinsic disease biology to optimize selection between ICI (single or double) and VEGF TKIs in treatment-naïve patients (NCT02960906).
Conclusion
Until ongoing clinical and translational investigations lead to the adoption of a composite panel of predictive biomarkers, the depth and duration of responses as well as clinical characteristics of the tumor and host will continue to guide next steps within this complex landscape.
Funding
This work was funded by the European Union and Greek national funds through the Operational Program Competitiveness, Entrepreneurship and Innovation, under the call RE-SEARCH—CREATE—INNOVATE, project code: T2EDK-03079.
Conflicts of Interest
The authors declare no conflicts of interest.
REFERENCES
1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022 Jan 72(1):7–33. 10.3322/caac.21708
2. SEER Stat fact sheets: Kidney and renal pelvis [Internet]. [cited
3. Kane CJ, Mallin K, Ritchey J, Cooperberg MR, Carroll PR. Renal cell cancer stage migration: Analysis of the national cancer data base. Cancer. 2008 Jul 1;113(1):78–83. 10.1002/cncr.23518
4. Tannir NM, Pal SK, Atkins MB. Second-line treatment landscape for renal cell carcinoma: A comprehensive review. Oncologist. 2018 May;23(5):540–55. 10.1634/theoncologist.2017-0534
5. Shamash J, Steele JP, Wilson P, Nystrom M, Ansell W, Oliver RT. IPM chemotherapy in cytokine refractory renal cell cancer. Br J Cancer. 2003 May 19;88(10):1516–21. 10.1038/sj.bjc.6600934
6. Rini BI, Plimack ER, Stus V, Gafanov R, Hawkins R, Nosov D, et al. Pembrolizumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2019 Mar 21;380(12):1116–27. 10.1056/NEJMoa1816714
7. Choueiri TK, Powles T, Burotto M, Escudier B, Bourlon MT, Zurawski B, et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2021 Mar 4;384(9):829–41. 10.1056/NEJMoa2026982
8. Motzer R, Alekseev B, Rha SY, Porta C, Eto M, Powles T, et al. Lenvatinib plus pembrolizumab or everolimus for advanced renal cell carcinoma. N Engl J Med. 2021 Apr 8;384(14):1289–300. 10.1056/NEJMoa2035716
9. Motzer RJ, Tannir NM, McDermott DF, Arén Frontera O, Melichar B, Choueiri TK, et al. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N Engl J Med. 2018 Apr 5;378(14):1277–90. 10.1056/NEJMoa1712126
10. Grimm MO, Leucht K, Foller S. Risk stratification and treatment algorithm of metastatic renal cell carcinoma. J Clin Med. 2021 Nov 16;10(22):5339. 10.3390/jcm10225339
11. Powles T, Albiges L, Bex A, Grünwald V, Porta C, Procopio G, et al. ESMO clinical practice guideline update on the use of immunotherapy in early stage and advanced renal cell carcinoma. Ann Oncol. 2021 Dec;32(12):1511–19. 10.1016/j.annonc.2021.09.014
12. Rizzo M, Porta C. Sunitinib in the treatment of renal cell carcinoma: An update on recent evidence. Ther Adv Urol. 2017 Jun 29;9(8):195–207. 10.1177/1756287217713902
13. Knox JJ, Barrios CH, Kim TM, Cosgriff T, Srimuninnimit V, Pittman K, et al. Final overall survival analysis for the phase II RECORD-3 study of first-line everolimus followed by sunitinib versus first-line sunitinib followed by everolimus in metastatic RCC. Ann Oncol. 2017 Jun 1;28(6):1339–45. 10.1093/annonc/mdx075
14. Oudard S, Geoffrois L, Guillot A, Chevreau C, Deville JL, Falkowski S, et al. Clinical activity of sunitinib rechallenge in metastatic renal cell carcinoma-results of the REchallenge with SUnitinib in MEtastatic RCC (RESUME) study. Eur J Cancer. 2016 Jul;62:28–35. 10.1016/j.ejca.2016.04.003
15. Grande E, Alonso-Gordoa T, Reig O, Esteban E, Castellano D, Garcia-Del-Muro X, et al. Results from the INMUNOSUN-SOGUG trial: A prospective phase II study of sunitinib as a second-line therapy in patients with metastatic renal cell carcinoma after immune checkpoint-based combination therapy. ESMO Open. 2022 Apr;7(2):100463. 10.1016/j.esmoop.2022.100463
16. Wells JC, Dudani S, Gan CL, Stukalin I, Azad AA, Liow E, et al. Clinical effectiveness of second-line sunitinib following immuno-oncology therapy in patients with metastatic renal cell carcinoma: A real-world study. Clin Genitourin Cancer. 2021 Aug;19(4):354–61. 10.1016/j.clgc.2021.03.006
17. Sternberg CN, Davis ID, Mardiak J, Szczylik C, Lee E, Wagstaff J, et al. Pazopanib in locally advanced or metastatic renal cell carcinoma: Results of a randomized phase III trial. J Clin Oncol. 2010 Feb 20;28(6):1061–8. 10.1200/JCO.2009.23.9764
18. Motzer RJ, Hutson TE, Cella D, Reeves J, Hawkins R, Guo J, et al. Pazopanib versus sunitinib in metastatic renal-cell carcinoma. N Engl J Med. 2013 Aug 22;369(8):722–31. 10.1056/NEJMoa1303989
19. Escudier B, Porta C, Bono P, Powles T, Eisen T, Sternberg CN, et al. Randomized, controlled, double-blind, cross-over trial assessing treatment preference for pazopanib versus sunitinib in patients with metastatic renal cell carcinoma: PISCES Study. J Clin Oncol. 2014 May 10;32(14):1412–18. 10.1200/JCO.2013.50.8267
20. Hainsworth JD, Rubin MS, Arrowsmith ER, Khatcheressian J, Crane EJ, Franco LA. Pazopanib as second-line treatment after sunitinib or bevacizumab in patients with advanced renal cell carcinoma: A Sarah Cannon Oncology Research Consortium Phase II trial. Clin Genitourin Cancer. 2013 Sep;11(3):270–5. 10.1016/j.clgc.2013.04.006
21. Bellmunt J, Esteban E, Del Muro XG, Sepúlveda JM, Maroto P, Gallardo E, et al. Pazopanib as second-line antiangiogenic treatment in metastatic renal cell carcinoma after tyrosine kinase inhibitor (TKI) failure: A phase 2 trial exploring immune-related biomarkers for testing in the post-immunotherapy/TKI era. Eur Urol Oncol. 2021 Jun;4(3):502–5. 10.1016/j.euo.2019.07.014
22. Kok VC, Kuo JT. Pazopanib as a second-line treatment for non-cytokine-treated metastatic renal cell carcinoma: A meta-analysis of the effect of treatment. BMC Urol. 2016 Jul 4;16(1):34. 10.1186/s12894-016-0156-4
23. Cao X, Tang D, Ratto B, Poole A, Ravichandran S, Jin L, et al. Real-world clinical outcomes of pazopanib immediately after discontinuation of immunotherapy for advanced renal cell carcinoma. Clin Genitourin Cancer. 2020 Feb;18(1):e37–45. 10.1016/j.clgc.2019.10.010
24. Escudier B, Eisen T, Stadler WM, Szczylik C, Oudard S, Staehler M, et al. Sorafenib for treatment of renal cell carcinoma: Final efficacy and safety results of the phase III treatment approaches in renal cancer global evaluation trial. J Clin Oncol. 2009 Jul 10;27(20):3312–18. 10.1200/JCO.2008.19.5511
25. Amzal B, Fu S, Meng J, Lister J, Karcher H. Cabozantinib versus everolimus, nivolumab, axitinib, sorafenib and best supportive care: A network meta-analysis of progression-free survival and overall survival in second line treatment of advanced renal cell carcinoma. PLoS One. 2017 Sep 8;12(9):e0184423. 10.1371/journal.pone.0184423
26. Rini BI, Escudier B, Tomczak P, Kaprin A, Szczylik C, Hutson TE, et al. Comparative effectiveness of axitinib versus sorafenib in advanced renal cell carcinoma (AXIS): A randomised phase 3 trial. Lancet. 2011 Dec 3;378(9807):1931–9. 10.1016/S0140-6736(11)61613-9
27. Motzer RJ, Escudier B, Tomczak P, Hutson TE, Michaelson MD, Negrier S, et al. Axitinib versus sorafenib as second-line treatment for advanced renal cell carcinoma: Overall survival analysis and updated results from a randomised phase 3 trial. Lancet Oncol. 2013 May;14(6):552–62. 10.1016/S1470-2045(13)70093-7
28. Cella D, Escudier B, Rini B, Chen C, Bhattacharyya H, Tarazi J, et al. Patient-reported outcomes for axitinib vs sorafenib in metastatic renal cell carcinoma: Phase III (AXIS) trial. Br J Cancer. 2013 Apr 30;108(8):1571–8. 10.1038/bjc.2013.145
29. Escudier B, Michaelson MD, Motzer RJ, Hutson TE, Clark JI, Lim HY, et al. Axitinib versus sorafenib in advanced renal cell carcinoma: Subanalyses by prior therapy from a randomised phase III trial. Br J Cancer. 2014 Jun 10;110(12):2821–8. 10.1038/bjc.2014.244
30. Bracarda S, Bamias A, Casper J, Negrier S, Sella A, Staehler M, et al. Is axitinib still a valid option for mRCC in the second-line setting? Prognostic factor analyses from the AXIS trial. Clin Genitourin Cancer. 2019 Jun 17(3):e689–703. 10.1016/j.clgc.2019.03.017
31. Tsimafeyeu I, Borisov P, Abdelgafur A, Leonenkov R, Novikova O, Guseva I, et al. Phase 2 multicenter single-arm study of second-line axitinib in favorable risk patients with metastatic renal cell carcinoma: FavorAx. Target Oncol. 2019 Feb;14(1):33–8. 10.1007/s11523-018-0613-y
32. Ornstein MC, Pal SK, Wood LS, Tomer JM, Hobbs BP, Jia XS, et al. Individualised axitinib regimen for patients with metastatic renal cell carcinoma after treatment with checkpoint inhibitors: A multicentre, single-arm, phase 2 study. Lancet Oncol. 2019 Oct;20(10):1386–94. 10.1016/S1470-2045(19)30513-3
33. Miyake H, Harada KI, Ozono S, Fujisawa M. Assessment of efficacy, safety, and quality of life of 124 patients treated with axitinib as second-line therapy for metastatic renal-cell carcinoma: Experience in real-world clinical practice in Japan. Clin Genitourin Cancer. 2017 Feb;15(1):122–8. 10.1016/j.clgc.2016.06.019
34. Santoni M, Iacovelli R, Colonna V, Klinz S, Mauri G, Nuti M. Antitumor effects of the multi-target tyrosine kinase inhibitor cabozantinib: A comprehensive review of the preclinical evidence. Expert Rev Anticancer Ther. 2021 Sep;21(9):1029–54. 10.1080/14737140.2021.1919090
35. Choueiri TK, Escudier B, Powles T, Tannir NM, Mainwaring PN, Rini BI, et al. Cabozantinib versus everolimus in advanced renal cell carcinoma (METEOR): Final results from a randomised, open-label, phase 3 trial. Lancet Oncol. 2016 Jul;17(7):917–27. 10.1016/S1470-2045(16)30107-3
36. Albiges L, Schmidinger M, Taguieva-Pioger N, Perol D, Grünwald V, Guemas E. CaboPoint: A phase II study of cabozantinib as second-line treatment in patients with metastatic renal cell carcinoma. Future Oncol. 2022 Mar;18(8):915–26. 10.2217/fon-2021-1006
37. Rini BI, Pal SK, Escudier BJ, Atkins MB, Hutson TE, Porta C, et al. Tivozanib versus sorafenib in patients with advanced renal cell carcinoma (TIVO-3): A phase 3, multicentre, randomised, controlled, open-label study. Lancet Oncol. 2020 Jan;21(1):95–104. 10.1016/S1470-2045(19)30735-1
38. Pal SK, Escudier BJ, Atkins MB, Hutson TE, Porta C, Verzoni E, et al. Final overall survival results from a phase 3 study to compare tivozanib to sorafenib as third-or fourth-line therapy in subjects with metastatic renal cell carcinoma. Eur Urol. 2020 Dec;78(6):783–5. 10.1016/j.eururo.2020.08.007
39. Motzer RJ, Hutson TE, Glen H, Michaelson MD, Molina A, Eisen T, et al. Lenvatinib, everolimus, and the combination in patients with metastatic renal cell carcinoma: A randomised, phase 2, open-label, multicentre trial. Lancet Oncol. 2015 Nov;16(15):1473–82. 10.1016/S1470-2045(15)00290-9
40. Pal SK, Puente J, Heng DYC, Glen H, Koralewski P, Stroyakovskiy D, et al. Assessing the safety and efficacy of two starting doses of lenvatinib plus everolimus in patients with renal cell carcinoma: A randomized phase 2 trial. Eur Urol. 2022;82(3):283–92. 10.1016/j.eururo.2021.12.024
41. Vogelzang NJ, Monnette AM, Wang Y, Wan Y, Xie Y, Robert NJ, et al. Real-world clinical effectiveness of lenvatinib/everolimus in a heavily pretreated advanced/metastatic renal cell carcinoma population in the US Community oncology setting. Clin Genitourin Cancer. 2021 Dec;19(6):531–9. 10.1016/j.clgc.2021.05.002
42. Motzer RJ, Escudier B, George S, Hammers HJ, Srinivas S, Tykodi SS, et al. Nivolumab versus everolimus in patients with advanced renal cell carcinoma: Updated results with long-term follow-up of the randomized, open-label, phase 3 CheckMate 025 trial. Cancer. 2020 Sep 15;126(18):4156–67. 10.1002/cncr.33033
43. Xu JX, Maher VE, Zhang L, Tang S, Sridhara R, Ibrahim A, et al. FDA approval summary: Nivolumab in advanced renal cell carcinoma after anti-angiogenic therapy and exploratory predictive biomarker analysis. Oncologist. 2017 Mar;22(3):311–17. 10.1634/theoncologist.2016-0476
44. Escudier B, Motzer RJ, Sharma P, Wagstaff J, Plimack ER, Hammers HJ, et al. Treatment beyond progression in patients with advanced renal cell carcinoma treated with nivolumab in CheckMate 025. Eur Urol. 2017 Sep;72(3):368–76. 10.1016/j.eururo.2017.03.037
45. Gul A, Stewart TF, Mantia CM, Shah NJ, Gatof ES, Long Y, et al. Salvage ipilimumab and nivolumab in patients with metastatic renal cell carcinoma after prior immune checkpoint inhibitors. J Clin Oncol. 2020 Sep 20;38(27):3088–94. 10.1200/JCO.19.03315
46. Vauchier C, Auclin E, Barthélémy P, Carril-Ajuria L, Ryckewaert T, Borchiellini D, et al. REchallenge of NIVOlumab (RENIVO) or nivolumab-ipilimumab in metastatic renal cell carcinoma: An ambispective multicenter study. J Oncol. 2022 Feb 18;2022:3449660. 10.1155/2022/3449660
47. Lee CH, Shah AY, Rasco D, Rao A, Taylor MH, Di Simone C, et al. Lenvatinib plus pembrolizumab in patients with either treatment-naive or previously treated metastatic renal cell carcinoma (study 111/KEYNOTE-146): A phase 1b/2 study. Lancet Oncol. 2021 Jul;22(7):946–58. 10.1016/S1470-2045(21)00241-2
48. Powles T, Atkins MB, Escudier B, Motzer RJ, Rini BI, Fong L, et al. Efficacy and safety of atezolizumab plus bevacizumab following disease progression on atezolizumab or sunitinib monotherapy in patients with metastatic renal cell carcinoma in IMmotion150: A randomized phase 2 clinical trial. Eur Urol. 2021 May;79(5):665–73. 10.1016/j.eururo.2021.01.003
49. Choueiri TK, Halabi S, Sanford BL, Hahn O, Michaelson MD, Walsh MK, et al. Cabozantinib versus sunitinib as initial targeted therapy for patients with metastatic renal cell carcinoma of poor or intermediate risk: The alliance A031203 CABOSUN trial. J Clin Oncol. 2017 Feb 20;35(6):591–7. 10.1200/JCO.2016.70.7398
50. Eichelberg C, Vervenne WL, De Santis M, Fischer von Weikersthal L, Goebell PJ, Lerchenmüller C, et al. SWITCH: A randomised, sequential, open-label study to evaluate the efficacy and safety of sorafenib-sunitinib versus sunitinib-sorafenib in the treatment of metastatic renal cell cancer. Eur Urol. 2015 Nov;68(5):837–47. 10.1016/j.eururo.2015.04.017
51. Motzer RJ, Barrios CH, Kim TM, Falcon S, Cosgriff T, Harker WG, et al. Phase II randomized trial comparing sequential first-line everolimus and second-line sunitinib versus first-line sunitinib and second-line everolimus in patients with metastatic renal cell carcinoma. J Clin Oncol. 2014 Sep 1;32(25):2765–72. 10.1200/JCO.2013.54.6911
52. Suzuki K, Terakawa T, Furukawa J, Harada K, Hinata N, Nakano Y, et al. Clinical outcomes of second-line treatment following prior targeted therapy in patients with metastatic renal cell carcinoma: A comparison of axitinib and nivolumab. Int J Clin Oncol. 2020 Sep;25(9):1678–86. 10.1007/s10147-020-01708-8
53. Suzuki K, Hara T, Terakawa T, Harada K, Fujisawa M. Efficacy of axitinib rechallenge in metastatic renal cell carcinoma. Int J Urol. 2021 Jun;28(6):702–3. 10.1111/iju.14529
54. Motzer RJ, Jonasch E, Agarwal N, Alva A, Baine M, Beckermann K, et al. Kidney cancer, version 3.2022, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2022 Jan 20(1):71–90. 10.6004/jnccn.2022.0001
55. Santoni M, Aurilio G, Massari F, Grande E, Matrana MR, Rizzo M, et al. Nivolumab VERSUS cabozantinib as second-line therapy in patients with advanced renal cell carcinoma: A real-world comparison. Clin Genitourin Cancer. 2022 Jun;20(3):285–95. 10.1016/j.clgc.2022.02.003
56. Brahmer JR, Drake CG, Wollner I, Powderly JD, Picus J, Sharfman WH, et al. Phase I study of single-agent anti-programmed death-1 (MDX-1106) in refractory solid tumors: Safety, clinical activity, pharmacodynamics, and immunologic correlates. J Clin Oncol. 2010 Jul 1;28(19):3167–75. 10.1200/JCO.2009.26.7609
57. Cogdill AP, Andrews MC, Wargo JA. Hallmarks of response to immune checkpoint blockade. Br J Cancer. 2017 Jun 27;117(1):1–7. 10.1038/bjc.2017.136
58. Waterhouse DM, Garon EB, Chandler J, McCleod M, Hussein M, Jotte R, et al. Continuous versus 1-year fixed-duration nivolumab in previously treated advanced non-small-cell lung cancer: CheckMate 153. J Clin Oncol. 2020 Nov 20;38(33):3863–73. 10.1200/JCO.20.00131
59. Jenkins RW, Barbie DA, Flaherty KT. Mechanisms of resistance to immune checkpoint inhibitors. Br J Cancer. 2018;118(1):9–16. 10.1038/bjc.2017.434
60. Sharma P, Hu-Lieskovan S, Wargo JA, Ribas A. Primary, adaptive, and acquired resistance to cancer immunotherapy. Cell. 2017;168 (4): 707–23. 10.1016/j.cell.2017.01.017
61. Vlachostergios PJ. Resistance to pembrolizumab and axitinib in renal cell carcinoma: Clinical and genomic evaluation. J Kidney Cancer VHL. 2020 Jun 2;7(1):7–11. 10.15586/jkcvhl.2020.135
62. Gobbini E, Charles J, Toffart AC, Leccia MT, Moro-Sibilot D, Giaj Levra M. Current opinions in immune checkpoint inhibitors rechallenge in solid cancers. Crit Rev Oncol Hematol. 2019 Dec;144:102816. 10.1016/j.critrevonc.2019.102816
63. Anagnostou V, Smith KN, Forde PM, Niknafs N, Bhattacharya R, White J, et al. Evolution of neoantigen landscape during immune checkpoint blockade in non-small cell lung cancer. Cancer Discov. 2017 Mar;7(3):264–76. 10.1158/2159-8290.CD-16-0828
64. Deeks ED. Belzutifan: First approval. Drugs. 2021 Nov;81(16):1921–7. 10.1007/s40265-021-01606-x
65. Bauer TM, Choueiri TK, Papadopoulos KP, Plimack ER, Merchan JR, McDermott DF, et al. The oral HIF-2 α inhibitor MK-6482 in patients with advanced clear cell renal cell carcinoma (RCC): Updated follow-up of a phase I/II study. J Clin Oncol. 2021;39(Suppl 6):273. 10.1200/JCO.2021.39.6_suppl.273
66. Choueiri TK, Bauer TM, Papadopoulos KP, Plimack ER, Merchan JR, McDermott DF, et al. Inhibition of hypoxia-inducible factor-2α in renal cell carcinoma with belzutifan: A phase 1 trial and biomarker analysis. Nat Med. 2021 May;27(5):802–5. 10.1038/s41591-021-01324-7
67. Benamran D, Albiges L, Bex A, Giannarini G, Capitanio U, Rouprêt M, EAU Section of Oncological Urology (ESOU) Board. Treatment options for De Novo metastatic clear-cell renal cell carcinoma: Current recommendations and future insights. Eur Urol Oncol. 2022 Feb;5(1):125–33. 10.1016/j.euo.2021.08.003
68. Donini M, Buti S, Massari F, Mollica V, Rizzo A, Montironi R, et al. Management of oligometastatic and oligoprogressive renal cell carcinoma: State of the art and future directions. Expert Rev Anticancer Ther. 2020 Jun;20(6):491–501. 10.1080/14737140.2020.1770601
69. Santini D, Ratta R, Pantano F, De Lisi D, Maruzzo M, Galli L, et al. Outcome of oligoprogressing metastatic renal cell carcinoma patients treated with locoregional therapy: A multicenter retrospective analysis. Oncotarget. 2017 Aug 7;8(59):100708–16. 10.18632/oncotarget.20022
70. Nagaraja H, Srivatsa N, Hemalatha S, Shweta S, Raghunath SK. Role of RPLND and metastasectomy in the management of oligometastatic renal cell carcinoma. Indian J Surg Oncol. 2018 Mar;9(1):105–9. 10.1007/s13193-018-0722-1
71. Meyer CP, Sun M, Karam JA, Leow JJ, de Velasco G, Pal SK, et al. Complications after metastasectomy for renal cell carcinoma—A population-based assessment. Eur Urol. 2017 Aug;72(2):171–4. 10.1016/j.eururo.2017.03.005
72. Sundet A, McConnell J, Walker K, Lindeque B. Intraoperative cryotherapy in the treatment of metastatic renal cell carcinoma of the bone. Orthopedics. 2021 Sep–Oct;44(5):e645–52. 10.3928/01477447-20210817-04
73. Bang HJ, Littrup PJ, Goodrich DJ, Currier BP, Aoun HD, Heilbrun LK, et al. Percutaneous cryoablation of metastatic renal cell carcinoma for local tumor control: Feasibility, outcomes, and estimated cost-effectiveness for palliation. J Vasc Interv Radiol. 2012 Jun;23(6):770–7. 10.1016/j.jvir.2012.03.002
74. Maciolek KA, Abel EJ, Best SL, Emamekhoo H, Averill SL, Ziemlewicz TJ, et al. Percutaneous microwave ablation for local control of metastatic renal cell carcinoma. Abdom Radiol (NY). 2018 Sep;43(9):2446–54. 10.1007/s00261-018-1498-z
75. Ali M, Mooi J, Lawrentschuk N, McKay RR, Hannan R, Lo SS, et al. The role of stereotactic ablative body radiotherapy in renal cell carcinoma. Eur Urol. 2022 Jul 14:S0302-2838(22)02468-X. 10.1016/j.eururo.2022.06.017
76. Masini C, Iotti C, De Giorgi U, Bellia RS, Buti S, Salaroli F, et al. Nivolumab in combination with stereotactic body radiotherapy in pretreated patients with metastatic renal cell carcinoma. Results of the phase II NIVES study. Eur Urol. 2022 Mar 81(3):274–82. 10.1016/j.eururo.2021.09.016
77. Pryor D, Bressel M, Lawrentschuk N, Tran B, Mooi J, Lewin J, et al. A phase I/II study of stereotactic radiotherapy and pembrolizumab for oligometastatic renal tumours (RAPPORT): Clinical trial protocol. Contemp Clin Trials Commun. 2021 Jan 6;21:100703. 10.1016/j.conctc.2021.100703
78. Kroeze SGC, Fritz C, Schaule J, Siva S, Kahl KH, Sundahl N, et al. Stereotactic radiotherapy combined with immunotherapy or targeted therapy for metastatic renal cell carcinoma. BJU Int. 2021 Jun;127(6):703–11. 10.1111/bju.15284
79. All S, Garant A, Hannan R. Stereotactic ablative radiation (SAbR) for oligometastatic RCC. Semin Radiat Oncol. 2021 Jul;31(3):227–34. 10.1016/j.semradonc.2021.02.002
80. Buti S, Bersanelli M, Viansone A, Leonetti A, Masini C, Ratta R, et al. Treatment outcome of metastatic lesions from renal cell carcinoma under going extra-cranial stereotactic body radioTHERapy: The together retrospective study. Cancer Treat Res Commun. 2020;22:100161. 10.1016/j.ctarc.2019.100161
81. Liu Y, Long W, Zhang Z, Zhang Z, Mai L, Huang S, et al. Metastasis-directed stereotactic body radiotherapy for oligometastatic renal cell carcinoma: Extent of tumor burden eradicated by radiotherapy. World J Urol. 2021 Nov;39(11):4183–90. 10.1007/s00345-021-03742-1
82. Franzese C, Marvaso G, Francolini G, Borghetti P, Trodella LE, Sepulcri M, et al. The role of stereotactic body radiation therapy and its integration with systemic therapies in metastatic kidney cancer: A multicenter study on behalf of the AIRO (Italian Association of Radiotherapy and Clinical Oncology) genitourinary study group. Clin Exp Metastasis. 2021 Dec;38(6):527–37. 10.1007/s10585-021-10131-w
83. Zhang Y, Schoenhals J, Christie A, Mohamad O, Wang C, Bowman I, et al. Stereotactic ablative radiation therapy (SAbR) used to defer systemic therapy in oligometastatic renal cell cancer. Int J Radiat Oncol Biol Phys. 2019 Oct 1;105(2):367–75. 10.1016/j.ijrobp.2019.07.023
84. Schoenhals JE, Mohamad O, Christie A, Zhang Y, Li D, Singla N, et al. Stereotactic ablative radiation therapy for oligoprogressive renal cell carcinoma. Adv Radiat Oncol. 2021 May 26;6(5):100692. 10.1016/j.adro.2021.100692
85. Meyer E, Pasquier D, Bernadou G, Calais G, Maroun P, Bossi A, et al. Stereotactic radiation therapy in the strategy of treatment of metastatic renal cell carcinoma: A study of the Getug group. Eur J Cancer. 2018 Jul;98:38–47. 10.1016/j.ejca.2018.04.008
86. De B, Venkatesan AM, Msaouel P, Ghia AJ, Li J, Yeboa DN, et al. Definitive radiotherapy for extracranial oligoprogressive metastatic renal cell carcinoma as a strategy to defer systemic therapy escalation. BJU Int. 2022 May;129(5):610–20. 10.1111/bju.15541
87. Tang C, Msaouel P, Hara K, Choi H, Le V, Shah AY, et al. Definitive radiotherapy in lieu of systemic therapy for oligometastatic renal cell carcinoma: A single-arm, single-centre, feasibility, phase 2 trial. Lancet Oncol. 2021 Dec;22(12):1732–9. 10.1016/S1470-2045(21)00528-3
88. Hannan R, Christensen M, Hammers H, Christie A, Paulman B, Lin D, et al. Phase II trial of stereotactic ablative radiation for oligoprogressive metastatic kidney cancer. Eur Urol Oncol. 2022 Apr;5(2):216–24. 10.1016/j.euo.2021.12.001
89. Cheung P, Patel S, North SA, Sahgal A, Chu W, Soliman H, et al. Stereotactic radiotherapy for oligoprogression in metastatic renal cell cancer patients receiving tyrosine kinase inhibitor therapy: A phase 2 prospective multicenter study. Eur Urol. 2021 Dec;80(6):693–700. 10.1016/j.eururo.2021.07.026
90. Barata PC, Mendiratta P, Kotecha R, Gopalakrishnan D, Juloori A, Chao ST, et al. Effect of switching systemic treatment after stereotactic radiosurgery for oligoprogressive, metastatic renal cell carcinoma. Clin Genitourin Cancer. 2018 Oct;16(5):413–19.e1. 10.1016/j.clgc.2018.07.018
91. Staehler M, Goebell PJ, Müller L, Emde TO, Wetzel N, Kruggel L, et al. Rare patients in routine care: Treatment and outcome in advanced papillary renal cell carcinoma in the prospective German clinical RCC-Registry. Int J Cancer. 2020 Mar 1;146(5):1307–15. 10.1002/ijc.32671
92. Hutson TE, Michaelson MD, Kuzel TM, Agarwal N, Molina AM, Hsieh JJ, et al. A single-arm, multicenter, phase 2 study of lenvatinib plus everolimus in patients with advanced non-clear cell renal cell carcinoma. Eur Urol. 2021 Aug;80(2):162–70. 10.1016/j.eururo.2021.03.015
93. Lee CH, Voss MH, Carlo MI, Chen YB, Zucker M, Knezevic A, et al. Phase II trial of cabozantinib plus nivolumab in patients with non-clear-cell renal cell carcinoma and genomic correlates. J Clin Oncol. 2022 Jul 20;40(21):2333–41. 10.1200/JCO.21.01944
94. Vogelzang NJ, Olsen MR, McFarlane JJ, Arrowsmith E, Bauer TM, Jain RK, et al. Safety and efficacy of nivolumab in patients with advanced non-clear cell renal cell carcinoma: Results from the phase IIIb/IV CheckMate 374 study. Clin Genitourin Cancer. 2020 Dec;18(6):461–8.e3. 10.1016/j.clgc.2020.05.006
95. Graham J, Wells JC, Dudani S, Gan CL, Donskov F, Lee JL, et al. Outcomes of patients with advanced non-clear cell renal cell carcinoma treated with first-line immune checkpoint inhibitor therapy. Eur J Cancer. 2022 Aug;171:124–32. 10.1016/j.ejca.2022.05.002
96. Tykodi SS, Gordan LN, Alter RS, Arrowsmith E, Harrison MR, Percent I, et al. Safety and efficacy of nivolumab plus ipilimumab in patients with advanced non-clear cell renal cell carcinoma: Results from the phase 3b/4 CheckMate 920 trial. J Immunother Cancer. 2022 Feb;10(2):e003844. 10.1136/jitc-2021-003844
97. McDermott DF, Lee JL, Ziobro M, Suarez C, Langiewicz P, Matveev VB, et al. Open-label, single-arm, phase II study of pembrolizumab monotherapy as first-line therapy in patients with advanced non-clear cell renal cell carcinoma. J Clin Oncol. 2021 Mar 20;39(9):1029–39. 10.1200/JCO.20.02365
98. Luzzago S, Palumbo C, Rosiello G, Knipper S, Pecoraro A, Mistretta FA, et al. Association between systemic therapy and/or cytoreductive nephrectomy and survival in contemporary metastatic non-clear cell renal cell carcinoma patients. Eur Urol Focus. 2021 May;7(3):598–607. 10.1016/j.euf.2020.04.009
99. Jonasch E, Donskov F, Iliopoulos O, Rathmell WK, Narayan VK, Maughan BL, et al. Belzutifan for renal cell carcinoma in von Hippel-Lindau disease. N Engl J Med. 2021 Nov 25;385(22):2036–46. 10.1056/NEJMoa2103425
100. Choueiri TK, Bauer TM, McDermott DF, Arrowsmith R, Roy A, Perini RF, et al. Phase 2 study of the oral hypoxia-inducible factor 2α (HIF-2α) inhibitor MK-6482 in combination with cabozantinib in patients with advanced clear cell renal cell carcinoma (ccRCC). J Clin Oncol. 2021;39(Suppl 6):272. 10.1200/JCO.2021.39.6_suppl.272
101. Tucker MD, Rini BI. Predicting response to immunotherapy in metastatic renal cell carcinoma. Cancers (Basel). 2020 Sep 18;12(9):2662. 10.3390/cancers12092662
102. Motzer RJ, Choueiri TK, McDermott DF, Powles T, Vano YA, Gupta S, et al. Biomarker analysis from CheckMate 214: Nivolumab plus ipilimumab versus sunitinib in renal cell carcinoma. J Immunother Cancer. 2022 Mar;10(3):e004316. 10.1136/jitc-2021-004316
103. Bi K, He MX, Bakouny Z, Kanodia A, Napolitano S, Wu J, et al. Tumor and immune reprogramming during immunotherapy in advanced renal cell carcinoma. Cancer Cell. 2021 May 10;39(5):649–61.e5. 10.1016/j.ccell.2021.02.015
104. Banchereau R, Leng N, Zill O, Sokol E, Liu G, Pavlick D, et al. Molecular determinants of response to PD-L1 blockade across tumor types. Nat Commun. 2021 Jun 25;12(1):3969. 10.1038/s41467-021-24112-w