
Download

Kidney Cancer: Case Reports
Partial Nephrectomy of Renal Cell Carcinoma in Horseshoe Kidney with Assistance of Intraoperative Retrograde Pyelogram: A Case Report and Literature Review
Omar Wai-kiu Tsui, Sunny Shek-long Tsang, Henry Hong-yin Lie, Thomas Ting-fung Wong, Wilson Pui-long Hung, Simon Hoi-lung Wong, Terence Chun-ting Lai, Chiu-fung Tsang*, Ada Tsui-lin Ng
Division of Urology, Department of Surgery, Queen Mary Hospital, the University of Hong Kong, Hong Kong
Abstract
Horseshoe kidney (HSK), characterized by the fusion of two kidneys forming a U-shape, presents intricate challenges in renal anatomy and poses a unique landscape for the development of renal cell carcinoma (RCC). This abstract delves into the case of a 74-year-old male with HSK who also developed RCC, where the employment of intraoperative retrograde pyelogram (RP) played a pivotal role in enhancing surgical precision. The patient’s complex tumor was successfully resected through meticulous identification and dissection. A comprehensive literature review reveals the significance of laparoscopic and robotic surgeries in treating RCC within HSKs, with 3D-reconstruction aiding in surgical planning. While advancements in imaging technologies have improved surgical outcomes, the underexplored utility of intraoperative RP stands out. RP provided real-time insights into the renal pelvis anatomy, guiding the surgical team in navigating intricate structures and ensuring optimal reconstruction post-tumor excision. The discussion underscores the challenges posed by RCC in HSKs, importance of preoperative 3D-reconstruction and angiography in surgical planning, and the critical role of intraoperative RP in mapping renal pelvis anatomy. Unlike conventional imaging methods, RP offers dynamic visualization of the renal drainage system, safeguarding against inadvertent closures and enhancing surgical precision. The successful utilization of RP in this case not only facilitated safe tumor resection but also highlighted its potential in managing unclear renal structures. In conclusion, the integration of intraoperative RP in surgical interventions for RCC within HSKs proves instrumental in enhancing surgical precision and navigating complex anatomical variations. By emphasizing the importance of real-time imaging guidance, surgeons can optimize treatment outcomes for individuals with RCC in the challenging context of HSK anomalies.
Key words: horseshoe kidney, partial nephrectomy, renal cell carcinoma, retrograde pyelogram, three-dimensional reconstruction
Received: 5 December 2025; Accepted after revision: 5 March 2026; Published: 23 March 2026
Author for correspondence: Chiu-fung Tsang, Division of Urology, Department of Surgery, Queen Mary Hospital, the University of Hong Kong, Hong Kong. Email: [email protected]
How to cite: Omar Wai-kiu Tsui et al. Partial Nephrectomy of Renal Cell Carcinoma in Horseshoe Kidney with Assistance of Intraoperative Retrograde Pyelogram: A Case Report and Literature Review. J Kidney Cancer VHL. 2026;13(1): 12–20.
Copyright: Omar Wai-kiu Tsui et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0
Introduction
Horseshoe kidney (HSK), a congenital anomaly where the two kidneys are fused at the lower ends forming a U-shape, presents a unique challenge in renal anatomy. This condition, arising during fetal development, can result in a range of potential complications affecting kidney function and overall urological health. With an estimated prevalence of about 0.25% among renal anomalies, HSK stands as a relatively rare occurrence (1). Research suggests a higher incidence in males compared to females, with a male-to-female ratio of approximately 2:1 (2). Though many individuals with this condition remain asymptomatic throughout their lives, some may encounter complications such as kidney stones, urinary tract infections, or structural abnormalities that require medical attention (3). Given the complexity and potential ramifications of HSK, close monitoring and management are crucial. Protection of remaining renal function in the solitary kidney is of utmost importance functionally in patients, while the oncological outcome of tumor resection is also crucial. Hence, image-guided preoperative assessments and intraoperative retrograde pyelogram (RP) plays important roles in achieving these aims.
Case Report
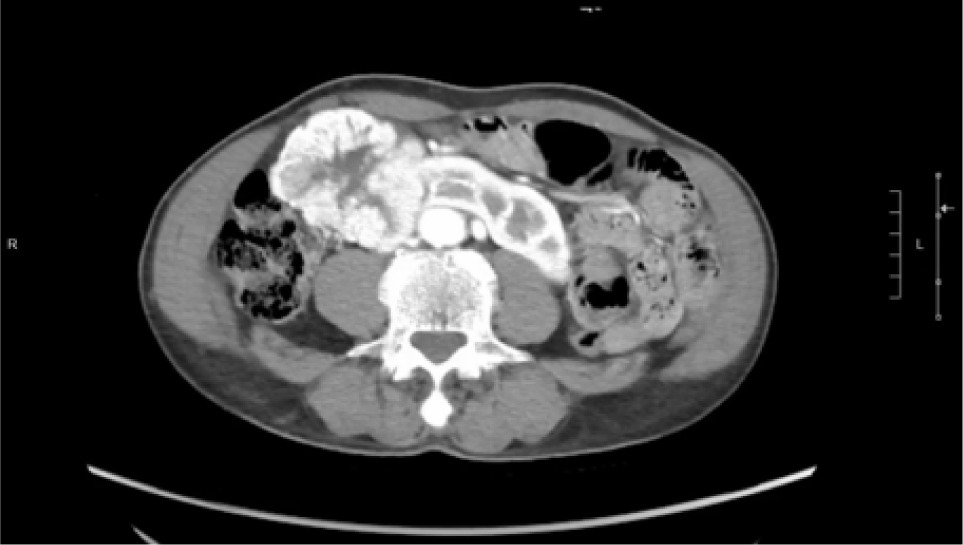
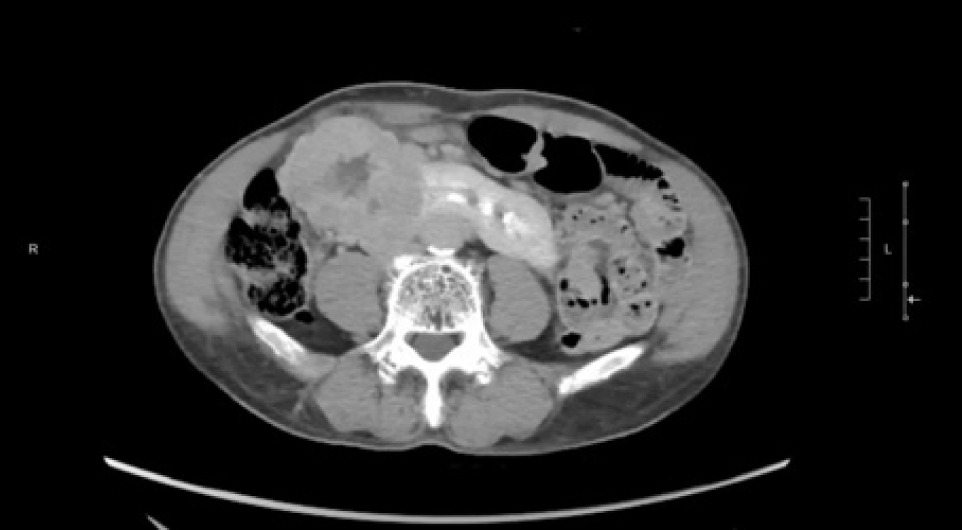
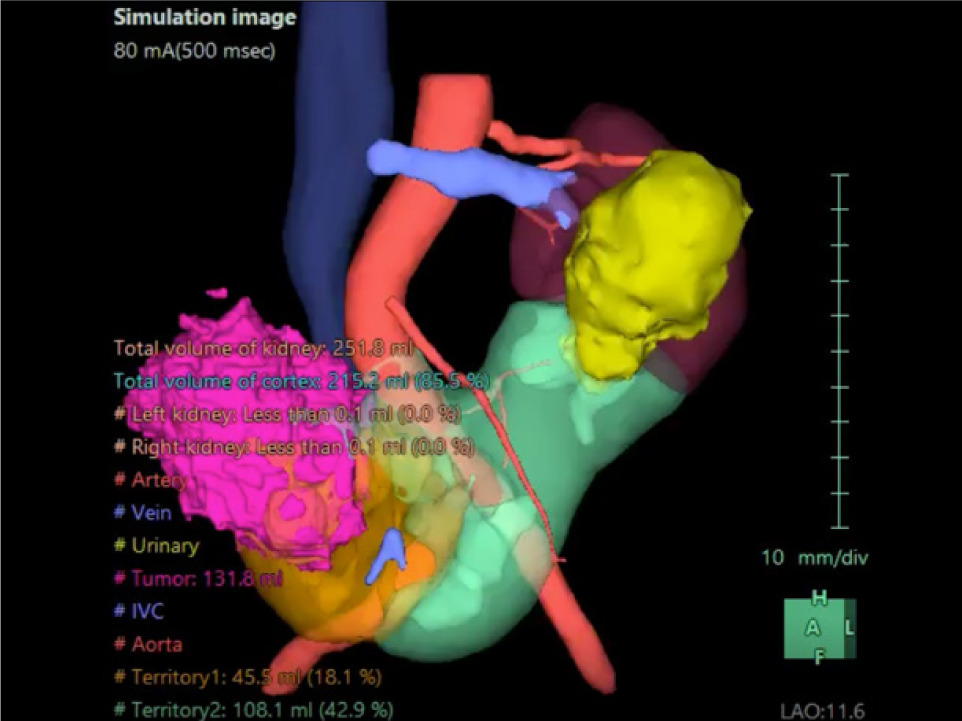
A 74-year-old Chinese male patient, ex-smoker, and social drinker, with a history of carcinoma of prostate in remission with laparoscopic radical prostatectomy done 11 years ago presented with an incidental finding of a right abdominal mass without frank symptoms. Preoperative eGFR ranges from 80 to 90 mL/min/1.73m2. Computed tomography (CT) showed a 7 cm heterogeneous mass on the right side of the HSK with complex hilar anatomy (Figures 1 & 2). Dual tracer (C-11 acetate and F18 FDG) positron emission tomography (PET-CT) showed moderate and mildly avid renal cell carcinoma (RCC) arising from HSK, without nodal or distant metastases. A 3D image reconstruction using FUJIFILM Synapse system was performed, showing complex tumor and vascular anatomy (two renal arteries and an additional artery to isthmus) (Figure 3). An open partial right nephrectomy was planned.
Figure 1: Axial cut of arterial phase-enhanced CT abdomen at the tumor level.
Figure 2: Axial cut of delayed phase-enhanced CT abdomen at the tumor level.
Figure 3: 3D reconstruction of horseshoe kidney and the tumor.
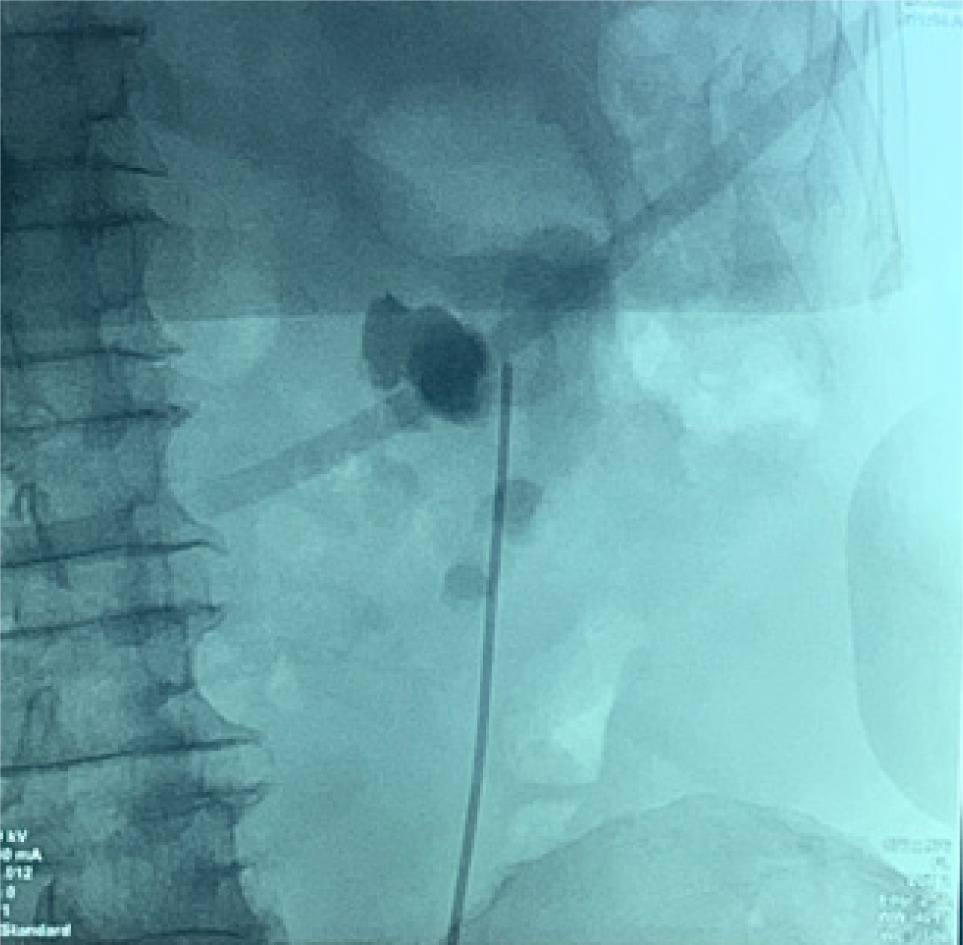
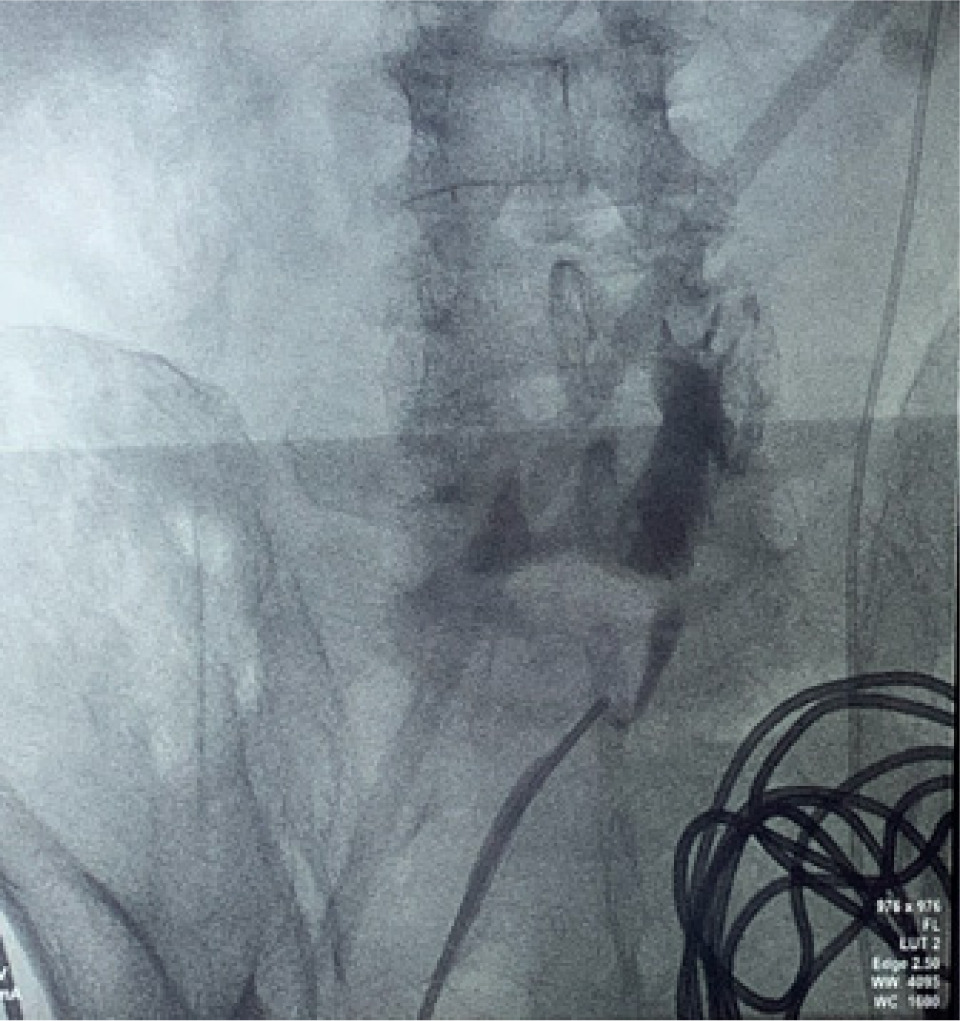
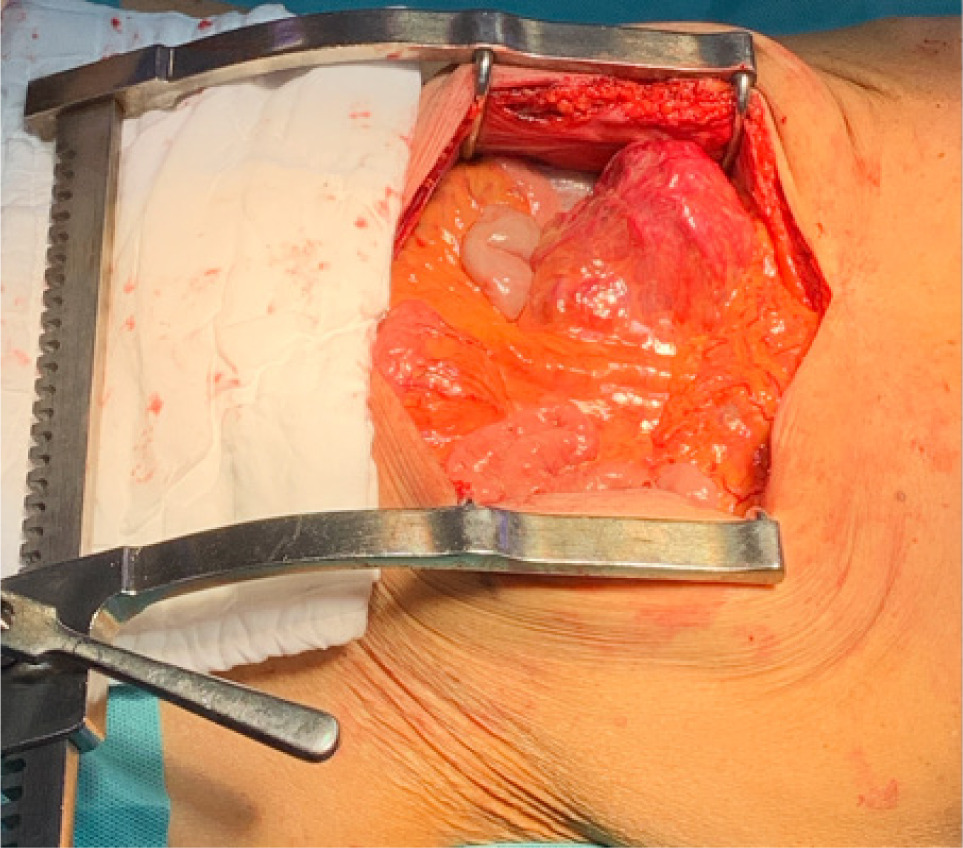
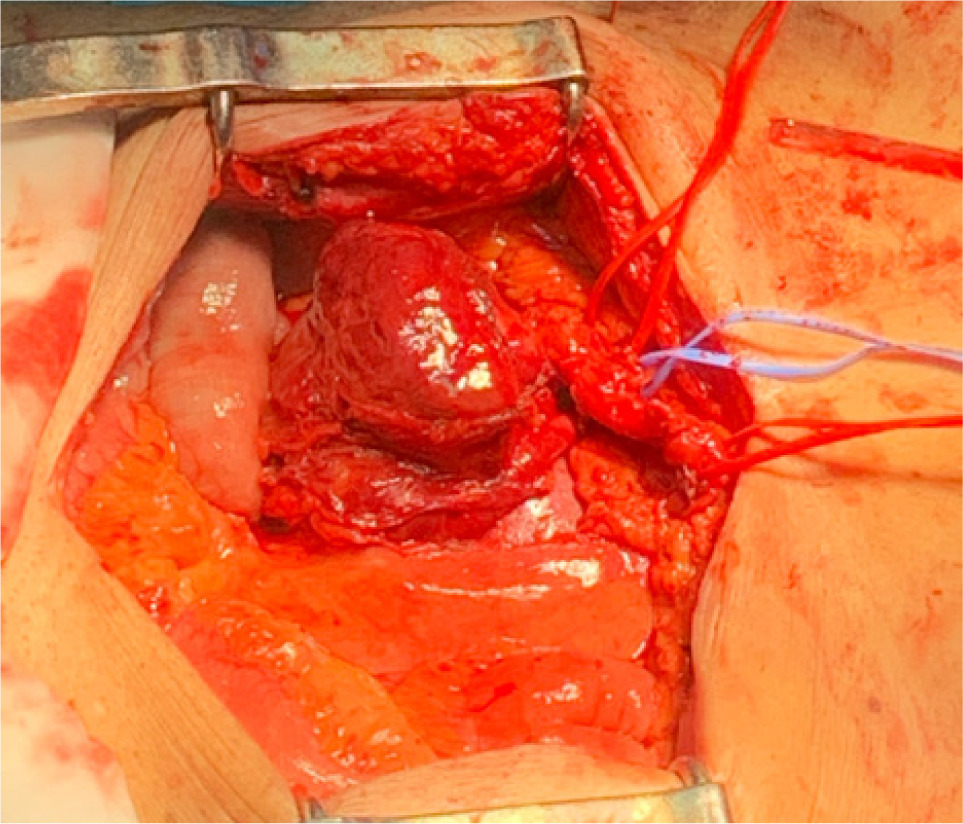
Bilateral RP and ureteric catheterization were first performed for the identification of the hila and calyces of the HSK (Figures 4 & 5). A lower midline laparotomy was performed. The tumor was identified, measuring 7 cm in diameter (Figure 6). Careful dissection of complex hilar structure was performed. Two renal arteries and two renal veins supplying the right side were identified and slung (Figure 7). The tumor was resected with artery clamping (Figure 8). The right lateral calyx of the pelvicalyceal (PC) system was involved and resected. The PC system was closed with 3/O PDS. Renorrhaphy was completed with 3/O V-Loc, and parenchyma was closed with 2/O V-Loc. Ischemic time was 20 minutes, and total operation time was 332 minutes. Blood loss was 420 mL. The patient had completed 1 week of levofloxacin and was discharged on postoperative day 6 with one kick of fever that spontaneously subsided.
Figure 4: Left renal pelvis.
Figure 5: Right renal pelvis.
Figure 6: Tumor before resection.
Figure 7: Carefully slung vasculatures.
Figure 8: Resected tumor.
Pathology report shows a 7.5 × 7 × 6.5 cm tumor of 113.2 g. On macroscopic examination, there were areas of hemorrhage and cystic change without gross perinephric tissue involvement. Microscopic examination shows clear cell RCC of WHO grade 2, with a pathological T2a staging. Surgical margin is clear.
Patient was followed up in 4 months’ time, and renal function was normal with no recurrence detected.
Literature review
We have reviewed 47 patients with renal tumor in HSK from multiple case reports; laparoscopic and robotic surgeries have similar clinical outcomes to open partial nephrectomy. Twenty patients (42.6%) are female, and 27 patients (57.4%) are male. The mean age is 53.93 years old (standard deviation (SD) 19.20 years old). The mean operative time is 197.85 minutes (SD 51.90 minutes), the mean ischemic time is 23.60 minutes (SD 10.77 minutes), and the mean blood loss is 235.56 mL (SD 172.35 mL). The average length of stay is 4.4 days (SD 2.70 days). Twenty patients (46.8%) have preoperative 3D reconstruction. Twenty-nine patients have RCC, five patients have primary carcinoid tumor, two patients each have oncocytoma and Wilm’s tumor, and one patient each has squamous cell carcinoma, angiomyolipoma, and hemangioma. In eight patients, the tumor type is not mentioned. Details of each case are presented in Table 1.
Table 1: Literature review on 3D preoperative reconstruction and intraoperative retrograde pyelogram.
| PMID | Age | Sex | Robot/Lap/Open/Nil | 3D recon. | Intraop RP | Operative time (mins) | Ischemic time (mins) | Blood loss (mL) | POD discharge | Complication | Tumor type |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 15679967 | 26 | F | Open | N | N | 30 | No recurrence at 8 months | Clear cell RCC | |||
| 16230165 | 52 | M | Open | N | N | 165 | 400 | ||||
| 17110020 | 62 | F | Laparoscopy | N | N | 210 | 70 | 3 | Oncocytoma | ||
| 17874547 | 52 | F | Open | N | N | Angiomyolipoma | |||||
| 19523243 | 50 | F | Nil | N | N | Primary carcinoid tumor | |||||
| 19588864 | 31 | M | Nil | N | N | Primary carcinoid tumor | |||||
| 19926945 | 59 | M | Nil | Y | N | Clear cell RCC | |||||
| 20801492 | 69 | M | Nil | N | N | SCC | |||||
| 22195272 | 21 | F | Laparoscopy | Y | N | 186 | 28 | 490 | |||
| 26766809 | 42 | F | Nil | Y | N | No recurrence at 7 months | Clear cell RCC | ||||
| 26892057 | 53 | M | Open, subcostal | N | N | 2 | Clear cell RCC | ||||
| 26892057 | 49 | F | Open, subcostal | N | N | 2 | Papillary RCC | ||||
| 26892057 | 50 | F | Open, subcostal | N | N | 2 | Primary carcinoid tumor, adenoCA | ||||
| 26892057 | 56 | M | Laparoscopy | N | N | 4 | Clear cell RCC | ||||
| 26892057 | 59 | F | Open, midline | N | N | 7 | Clear cell RCC | ||||
| 26892057 | 86 | F | Open, midline | N | N | 5 | Clear cell RCC | ||||
| 26892057 | 60 | M | Open, midline | N | N | 7 | Clear cell RCC | ||||
| 26892057 | 66 | M | Open, midline | N | N | 3 | Clear cell RCC | ||||
| 26948529 | 5 | F | Open | N | N | Wilm’s tumor | |||||
| 28245540 | 79 | M | Open | Y | N | 200 | 12 | 380 | Clear cell RCC | ||
| 28435792 | 69 | M | Laparoscopy | Y | N | 156 | 24 | 75 | 4 | No recurrence at 6 months | Clear cell RCC |
| 29288785 | 53 | F | Robot-assisted laparoscopy | Y | N | 170 | 150 | 2 | Oncocytoma | ||
| 29473385 | 37 | F | Open | N | N | Clear cell RCC | |||||
| 29977636 | 83 | F | Laparoscopy | N | N | 159 | 11 | 11 | No recurrence at 43 months | Clear cell RCC | |
| 30357753 | 51 | F | Laparoscopy | N | N | Primary carcinoid tumor | |||||
| 31808400 | 53 | M | Laparoscopy | Y | N | RCC | |||||
| 32489122 | 65 | M | Laparoscopic | Y | N | 210 | 30 | 370 | No recurrence at 24 months | Clear cell RCC | |
| 32743445 | 66 | M | Robot-assisted laparoscopy | Y | N | 295 | 13 | 100 | 7 | No recurrence at 6 months | Clear cell RCC |
| 32775638 | 55 | F | Laparoscopy | Y | N | 208 | 200 | No recurrence at 3 months | Clear cell RCC | ||
| 32775638 | 50 | M | Laparoscopy | Y | N | 225 | 28 | 350 | No recurrence at 12 months | Clear cell RCC | |
| 33990296 | 50 | M | Open | Y | N (used USG) | No recurrence at 6 and 12 months | RCC (grade II) | ||||
| 34258538 | 84 | F | Robot-assisted laparoscopy | Y | N | 185 | 18 | 8 | Clear cell RCC | ||
| 34326031 | 82 | M | Laparoscopy | Y | N | 2 | |||||
| 34326031 | 64 | M | Laparoscopy | Y | N | 2 | |||||
| 34521468 | 9 | M | Nil | N | N | Wilm’s tumor | |||||
| 35725279 | 60 | M | Laparoscopy | N | N | 53 | Chromophobe RCC | ||||
| 35727421 | 71 | F | Laparoscopy | Y | N | 135 | 25 | 80 | 6 | Hemangioma | |
| 35795128 | 75 | M | Laparoscopy | N | N | 225 | 18 | No recurrence at 3 months | Clear cell RCC | ||
| 37275562 | 19 | M | Robot-assisted laparoscopy | N | N | 140 | 170 | 3 | SDH-deficient RCC | ||
| 37275562 | 19 | M | Robot-assisted laparoscopy | N | N | 160 | 600 | 1 | SDH-deficient RCC | ||
| 37908786 | 41 | M | Open | N | N (used USG) | 215 | 200 | 7 | No recurrence at 16 months | Clear cell RCC | |
| 38178790 | 74 | M | Robot-assisted laparoscopy | Y | N | ||||||
| 38233275 | 42 | M | Laparoscopy | Y | RCC | ||||||
| 38711819 | 65 | F | Robot-assisted laparoscopy | Y | N | 355 | 19 | No recurrence at 6 months | Primary carcinoid tumor | ||
| 38936940 | 61 | M | Robot-assisted laparoscopy | Y | N | 181 | 14 | 100 | No recurrence at 53 months | Clear cell RCC | |
| 38936940 | 45 | F | Robot-assisted laparoscopy | Y | N | 177 | 31 | 34 | No recurrence at 13 months | Clear cell RCC | |
| 39914014 | 65 | M | Nil | Y | N | No recurrence at 52 months |
Note: Y = yes; N = no; Lap = laparoscopy; Nil = not mentioned; Intraop RP = Intraoperative retrograde pyelogram; 3D recon. = 3-dimensional reconstruction; POD discharge = postoperative day discharge; RCC = renal cell carcinoma; SCC = squamous cell carcinoma.
Based on the findings from the literature review, laparoscopic and robotic surgeries have emerged as sophisticated approaches for treating tumors in HSKs. Notably, approximately half of the cases incorporate 3D-reconstruction, underscoring the established efficacy of this technique in orchestrating surgeries involving intricate anatomy. However, despite these advancements, none of the studies have documented the utilization of intraoperative retrograde pyelography (RP). In contrast, RP offers real-time insights into the renal pelvis anatomy and its drainage system, equipping surgeons with invaluable details on the complexities of renal pelvis anatomy. This dynamic tool not only furnishes immediate feedback on the viability of renal pelvis reconstruction post-tumor excision but also averts the risk of inadvertent closure of the drainage system following reconstruction, thereby enhancing surgical precision and postoperative outcomes.
Discussion
RCC is the most common (around 90%) type of kidney cancer and can arise within the renal tissue of an HSK (4). While upper tract transitional cell carcinoma accounts for 5–10% of all transitional cell carcinoma, and renal sarcoma accounts for <1% of renal tumor (6). The challenges posed by RCC in individuals with HSK are similar to those faced by individuals with RCC in normal kidney anatomy. Early detection and appropriate management of RCC in individuals with HSK are essential to mitigate the risks associated with this complication and improve patient outcomes.
Surgical challenges encountered when treating RCC in a HSK can be notably complex, particularly due to the presence of aberrant vascular structures surrounding the tumor (7). To address these intricacies effectively, preoperative 3D reconstruction of the HSK is imperative to safeguard delicate structures during the surgical intervention (8), as well as preoperative angiography (9). Intraoperatively, the meticulous identification and careful dissection along these vascular structures with the usage of RP is paramount to prevent complications such as solitary kidney ischemia and potential risks like ischemic bowel.
HSK has variable arterial blood supply and vessel size. Injury to arteries and their branches in HSK can cause ischemia and deterioration in renal function (9). Pre-operative angiography is widely used among renal transplant cases and trauma patients, allowing urologists to visualize vessels to protect (10). Preoperative HSK angiography can aid surgical precision in terms of protection of significant vessels from being damaged. Other imaging modalities can also serve similar purposes, such as CT angiography (11). Along with 3D reconstruction, preoperative angiography can aid surgeons to remove the tumor precisely while not disturbing significant vessels, in order to achieve the highest remaining renal parenchyma (RRP), aiming more than 50% of the remaining HSK parenchyma (12).
Moreover, challenges may arise when conventional imaging methods such as CT scans and 3D reconstructions fail to provide a clear depiction of the renal pelvis, leading to uncertainties regarding its boundaries and internal structure. In such instances, intraoperative strategies become crucial, including RP of the renal pelvis and collecting system to guide surgical decision-making. In addition, the intraoperative injection of the dye can be utilized to confirm the precise location of the renal pelvis, aiding in surgical navigation. Real-time imaging techniques using fluoroscopy at key junctures in the procedure, such as before making incisions, prior to tumor removal, and after closing the renal pelvis, offer valuable insights and guidance in managing the unclear structures effectively. Employing on-table surgical planning based on real-time imaging data becomes essential in adapting to unforeseen challenges and ensuring optimal treatment outcomes for RCC within the unique anatomical context of an HSK.
We have effectively utilized intraoperative RP to enhance surgical precision in mapping the intricate anatomy of the renal pelvis. Unlike previous methods relying on CT scans and 3D reconstructions, which often fall short in detailing the exact drainage pathways from the renal pelvis to the ureters in cases of HSKs, intraoperative RP provides invaluable insights. This technique enables our surgical team to gain a comprehensive understanding of the renal drainage system, crucial for ensuring that the renal pelvis remains open and connected to the appropriate structures following partial nephrectomy. In essence, intraoperative RP serves as a vital and secure tool for urologists, empowering them to navigate the complexities surrounding anomalous renal pelvis structures with precision, thereby mitigating the risks of postoperative complications.
Preoperative 3D reconstruction and angiogram, along with intraoperative RP, provide the safest surgical planning and operation to patients, securing renal function, RRP, and ensuring oncological outcome.
Conclusion
In conclusion, the intricate case of the 74-year-old male patient with HSK and RCC highlights the challenges and complexities faced in managing RCC within this congenital anomaly. Surgical interventions necessitated precise planning, meticulous intraoperative techniques, and utilization of advanced imaging modalities to navigate the unique anatomical intricacies of the HSK. The successful enucleation of the tumor amidst complex vascular structures and ambiguous renal pelvis anatomy underscores the importance of tailored approaches in addressing RCC within such atypical renal configurations. Intraoperative RP provides real-time image guidance for surgical safety and information of dynamic renal pelvis drainage system. Multidisciplinary collaboration, personalized care strategies, and real-time imaging guidance played pivotal roles in ensuring optimal surgical outcomes and effective management of RCC in this specialized context. By emphasizing a patient-centered approach and leveraging cutting-edge technologies, healthcare providers can enhance treatment efficacy and quality of care for individuals with RCC in the challenging setting of HSK anomalies.
Mandatory Disclosure on Use of Artificial Intelligence
The authors declare that no AI-assisted tools were used in the preparation of this manuscript. All references have been manually verified for accuracy and relevance.
Acknowledgements
All clinical figures and photos are taken with the full consent of the patient.
We are grateful to the patient for consenting to publishing this case report for scientific and research purposes.
Author Contributions
Concept or design: OWK Tsui, CF Tsang; Acquisition of data: OWK Tsui, WPL Hung, CF Tsang; Analysis or interpretation of data: OWK Tsui; Drafting of the manuscript: OWK Tsui, SL Tsang; Critical revision of the manuscript for important intellectual content: All authors.
Conflict of Interest
None.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
REFERENCES
1. Chaabouni Y, Guesmi R, Hentati Y, Kammoun K, Hmida MB, Mnif Z, et al. Minimal change disease in horseshoe kidney. Pan African Medical Journal. 2017 Apr; 28; 26:243. 10.11604/pamj.2017.26.243.11438
2. Kirkpatrick JJ and Leslie SW. Horseshoe Kidney. 2023 May 30. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMid: 28613757. Available at: https://www.ncbi.nlm.nih.gov/books/NBK431105/
3. Nechita OC, Badescu D, Popescu RI, Rascu S, Petca RC, Aurelian J, et al. Reviewing the complexities of horseshoe kidney: insights into embryogenesis and surgical considerations. Journal of Medicine and Life. 2025 Jan;18(1):10–19. 10.25122/jml-2024-0325
4. Pandey J, Syed W. Renal Cancer. 2024 Oct 4. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026.
5. Green DA, Rink M, Xylinas E, Matin SF, Stenzl A, Roupret M, et al. Urothelial carcinoma of the bladder and the upper tract: disparate twins. Journal of Urology. 2013 Apr;189(4):1214–21. 10.1016/j.juro.2012.05.079. Epub 2012 Sep 27. PMid: 23023150.
6. Alevizakos M, Gaitanidis A, Korentzelos D, Basourakos SP, Burgess M. Renal sarcoma: A population-based study. Clinical Genitourinary Cancer. 2023 Feb;21(1):155–161. 10.1016/j.clgc.2022.07.012
7. Chaker K, Gharbia N, Ouanes Y, Zehani A, Mosbahi B, Nouira Y. Renal cell carcinoma in a horseshoe kidney: a case report. International Journal of Surgery Case Reports. 2025 Mar;128:111015. 10.1016/j.ijscr.2025.111015
8. Zhang Z, Wang H, Xiao Y, Zhang H, Huang Z. Laparoscopic nephron-sparing surgery for horseshoe kidney complicated with renal hemangioma: a case report and literature review. Clinical and Experimental Nephrology Case Reports 2023 Feb;12(1):23–26. 10.1007/s13730-022-00712-3
9. Zarfati A, Rollo G, Cassanelli G, Grimaldi C, Persano G, Natali GL, et al. The impact of pre-operative angiography on nephron-sparing surgery and outcome in Wilms tumor arising from horseshoe kidney: case report and literature review. Frontiers in Surgery. 2025 Apr 8;12:1528438. 10.3389/fsurg.2025.1528438
10. Neville C, House AA, Nguan CY, Beasley KA, Peck D, Thain LM, et al. Prospective comparison of magnetic resonance angiography with selective renal angiography for living kidney donor assessment. Urology. 2008 Mar;71(3):385–9. 10.1016/j.urology.2007.10.030
11. Xiong BJ, Yu Y, Wang X, Tao GJ, Xie JK, Lei T. Renal cell carcinoma in horseshoe kidney treated with retroperitoneoscopic partial nephrectomy: a case report. Urology Case Reports. 2025 Mar 24;60:103025. 10.1016/j.eucr.2025.103025
12. Rollo G, Zarfati A, Martucci C, Crocoli A, Serra A, Inserra A. Nephron-sparing surgery in pediatric renal tumors arising from a horseshoe kidney: proposal of a lacking definition. Journal of Pediatric Surgery. 2024 Jul;59(7):1404–1405. 10.1016/j.jpedsurg.2024.03.035